
Abstract
Skin cancer represents a significant global health burden, with over 380,000 new cases diagnosed annually. Convolutional neural networks (CNNs) have emerged as a promising tool to support skin cancer screening, yet evidence across diagnostic, economic and implementation domains remains fragmented. This review synthesises evidence on the diagnostic accuracy, real-world effectiveness, health economic implications, qualitative implementation considerations and ethical dimensions of AI-assisted skin cancer screening. CNNs demonstrate diagnostic performance comparable to dermatologists for common pigmented lesions, though accuracy declines markedly for rare subtypes and real-world settings. Health economic evidence is limited and context dependent. Qualitative evidence highlights cautious stakeholder optimism for AI-supported primary care triage, while pervasive algorithmic bias stemming from non-representative training datasets raises serious ethical concerns regarding beneficence, autonomy and justice. We conclude that safe and equitable implementation requires diverse, real-world validation studies and context-specific cost-effectiveness analyses to guide sustainable adoption.
1. Introduction
Skin cancer is a collective term for a heterogeneous group of malignant neoplasms that arise from cells within the skin rather than a single disease entity (Hasan et al., 2023). Its two major categories are melanoma and keratinocyte carcinomas (Hasan et al., 2023). Although rare, merkel cell carcinoma (MCC) is also recognised as a distinct form of non-melanoma skin cancer (Hasan et al., 2023). Melanoma develops through the malignant transformation of melanocytes: the cells that give the skin its pigmentation (Hasan et al., 2023). In contrast, keratinocyte carcinomas develop from epidermal keratinocytes, including the cutaneous squamous cell carcinoma (SCC) and basal cell carcinoma (BCC) (Hasan et al, 2023). While keratinocyte carcinomas represent most cases and are less aggressive, both basal cell carcinoma and squamous cell carcinoma have the potential to invade locally and metastasise (albeit very rare for BCC) (Raky et al., 2025). Melanomas exhibit a significantly higher risk of metastasis and account for most skin cancer-related deaths (Raky et al., 2025).
1.1 Epidemiology of skin cancer: prevalence, incidence and at-risk populations
Skin cancer is the most commonly diagnosed group of cancers worldwide (Arnold et al., 2022). In 2020, there were an estimated 325,000 new melanoma cases and 57,000 deaths globally (Arnold et al., 2022). Incidence was highest in Australia and New Zealand, reaching 42 and 31 cases per 100,000 person-years in males and females, respectively, in comparison to 1 case per 100,000 person-years in most African and Asian regions (Arnold et al., 2022). Melanoma is more common among males, older adults and fair-skinned populations of European descent because of greater vulnerability to ultraviolet radiation (Arnold et al., 2022). Keratinocyte carcinomas are more common, although their prevalence is difficult to estimate because basal cell and cutaneous squamous cell carcinomas are often incompletely recorded and individuals may develop multiple tumours (Nagarajan et al., 2019). The risk of keratinocyte carcinoma is also associated with older age, cumulative ultraviolet exposure, fair skin and immunosuppression (Nagarajan et al., 2019).
1.2 Societal costs of skin cancer: economics, premature mortality and morbidity
In recent years, there has been increasing recognition of skin cancer as a significant economic burden on society, in addition to the morbidity and mortality associated with the malignancies. In 2008, a research group estimated the annual cost of skin cancer to be at €142.2 million in Sweden (Eriksson & Tinghög, 2014). This estimate included both melanoma and non-melanoma forms of skin cancer and was based on both direct medical costs and indirect medical costs in terms of lost productivity due to sickness and premature death (Eriksson & Tinghög, 2014). Beyond its economic costs, skin cancer also causes premature mortality and morbidity in the Global Burden of Disease Study (GBD) (Kocarnak et al., 2019). Premature mortality was measured using years of life lost, while non-fatal health loss was measured using years lived with disability. The study estimated that malignant melanoma caused approximately 62,800 deaths worldwide in 2019, while non-melanoma skin cancer caused around 56,100 deaths (Kocarnak et al., 2019). It also estimated 290,000 new melanoma cases and 6.35 million new cases of non-melanoma skin cancer, demonstrating that the burden of skin cancer extends beyond healthcare expenditure and productivity loss (Kocarnak et al., 2019).
1.3 Artificial intelligence and CNNs for image analysis
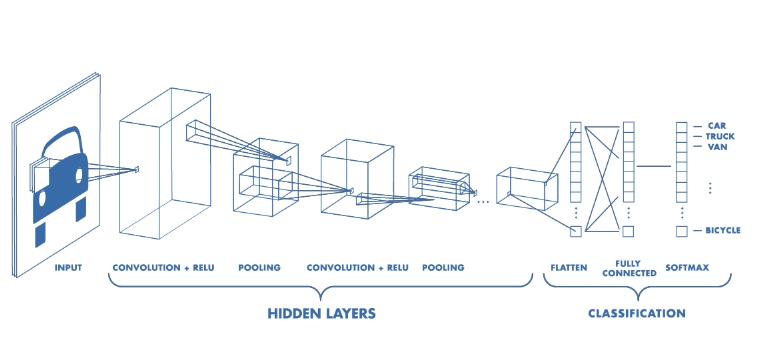
Artificial intelligence (AI) can be defined as the ability of a machine to perform tasks that usually require human intelligence (Stajic et al., 2015). Machine learning is a branch of AI in which computer algorithms learn patterns from data and improve performance through experience (Stajic et al., 2015). Deep learning is a specialised form of machine learning that uses multilayered artificial neural networks to identify complex relationships between input data and their corresponding labels (Fan et al., 2021). Convolutional neural networks (CNNs) are deep learning algorithms commonly used for image classification, segmentation and object detection (Purwono et al., 2022). A CNN consists of convolutional, pooling, fully-connected and non-linear layers. The convolutional layer uses kernel filters to extract fundamental features from an input image, while the pooling layer reduces the dimensions of the resulting feature maps (Purwono et al., 2022). The fully-connected layer then uses these extracted features to generate the final output (Purwono et al., 2022).
Esteva et al. (2017) demonstrated the potential of CNNs for automated skin cancer classification by training a network on 129,450 clinical images representing 2,032 skin diseases and comparing its performance with 21 board-certified dermatologists. Under the study’s experimental conditions, the CNN achieved performance comparable to that of dermatologists when distinguishing malignant melanoma from benign naevi and keratinocyte carcinomas from benign lesions (Esteva et al., 2017). Similarly, Haenssle et al. (2018) compared an Inception-v4 CNN with 58 dermatologists using dermoscopic images of melanocytic lesions and found that the CNN achieved greater specificity at the dermatologists’ mean sensitivity. However, both studies used retrospective, selected image sets, meaning that their findings demonstrate emerging diagnostic potential rather than proven effectiveness in routine clinical practice (Esteva et al., 2017; Haenssle et al., 2018).
1.4 The scope of this review
This paper aims to review the evidence regarding limitations and opportunities of using AI in skin cancer screening. Specifically, we will explain the diagnostic accuracy, real-world effectiveness, health economic implications, implementation strategies and ethical considerations of using CNNs in skin cancer screening across a range of contexts.
2. Diagnostic Accuracy
2.1 How CNNs work
CNNs are deep learning models designed mainly for image analysis (Purwono et al., 2022). A CNN interprets images as a matrix of numerical pixel values rather than how humans see images (Purwono et al., 2022). In the convolutional layer, small filters called kernels slide across the image and detect features such as edges, colour and texture (Purwono et al., 2022). Activation functions allow the network to learn complex, non-linear patterns, while the pooling layers reduce the size of the feature maps and lower computational requirements (Purwono et al., 2022). The extracted information is then passed to the fully connected layer, which then assigns probabilities to possible classifications (Purwono et al., 2022). CNN architectures differ in their depth, number and engagement of layers, filter sizes and computational demands (Purwono et al., 2022). For example, LeNet is shallow, whereas AlexNet and VGGNet contain more convolutional layers and can learn increasingly complex visual features (Purwono et al., 2022).
(Purwono et al., 2022)
2.2 How CNNs are tested: images and datasets
CNNs are tested using images that were not used during training because the model must be evaluated on whether it can classify unseen cases rather than memorise training examples (Purwono et al., 2022). In skin cancer research, the images are usually dermoscopic images. Esteva et al (2017) trained a CNN on 129,450 clinical images covering 2,032 diseases and tested it against 21 board-certified dermatologists using biopsy-proven clinical images. Another major dataset is HAM10000, which contains 10,015 dermoscopic images of pigmented skin lesions and was released through the ISIC archive for academic machine-learning research (Tschandl et al., 2018). Reference diagnoses in HAM10000 were established through pathology, follow-up, expert consensus or confocal microscopy (Tschandl et al., 2018). CNN performance can also be compared directly with dermatologists, as Haenssle et al., (2018) compared a CNN with 58 dermatologists for dermoscopic melanoma recognition.
When evaluating the accuracy of existing CNNs, sensitivity (ability to detect true positives) and specificity (ability to detect true negatives) measurements are taken. Accuracy tests differentiate in the stage of skin cancer tested as well as the neural network’s programming. Papachristou et al. (2024) evaluated the Dermalyser app programmed with machine learning algorithms and reported a sensitivity of 100% and specificity of 92.6% for detecting invasive melanomas. Comparatively, the same app in differentiating melanoma from nonmelanoma lesions corresponded to a 95.2% sensitivity and 84.5% specificity (Papachristou et al., 2024). The same software has a change in accuracy due to the type of detection that was screened (Papachristou et al., 2024).
Developing the CNNs requires a representative dataset as well as high numbers of images. For example, a deep learning algorithm for the detection of melanoma using 111 dermoscopy images compared to 1,010 dermoscopy images increased an AUC from 0.91 to 0.94 (Esteva et al., 2017). Because app usage by patients indicates reliance on varying phone camera qualities to accurately detect lesion concerns, this could impact AI’s diagnostic accuracy in real-world settings compared to testing models on dermoscopy datasets. Since the paper’s publishing in 2017, there is now a larger number of images available to train models with, which would increase accuracy due to higher incidence rates and mortality observed (Haenssle et al., 2018).
Similar findings by Haenssle et al. (2018) support dermatologists’ increased performance in detection accuracy with more clinical information. This is seen from 86.6% sensitivity and 71.3% specificity increasing to 88.9% sensitivity and 75.7% specificity with greater information for diagnosis (Haenssle et al., 2018). The Google Inception v4 CNN architecture was trained to compare AI and specialist performance and delivered a higher specificity of 82.5% and a greater AUC value than the accuracy of dermatologists with dermoscopy images, clinical information and images (Haenssle et al., 2018). In the line of medical accuracy, primary care physicians have a sensitivity ranging from 50-84% and specificity of 71-89% compared to dermatologist detection at a sensitivity ranging from 73-96% and specificity of 73-98% (Papachristou et al., 2024). Specialists and AI screening have higher percentage accuracies in skin cancer detection than nonspecialists (Papachristou et al., 2024). Distant imagery is not the only way lesions are studied, and lab-based studies testing AI’s diagnostic accuracy only rely on image comparison. Consequently, this data may overestimate AI’s performance compared to real-world usage.
Previous to testing AI’s role in skin cancer detection, noninvasive and histopathologic tissue analysis methods were used by dermatologists. Histopathologic analysis is considered the gold standard in a process where tissue is removed and examined for abnormalities by a pathologist (Heibel et al., 2020). Contact images have higher levels of specificity than distant images but stay equal at 73% sensitivity (Carli et al., 2002). Noninvasive imaging techniques reduce unnecessary biopsies, patient anxiety and healthcare costs while maintaining high diagnostic sensitivity. Their effectiveness does remain dependent on dermatologist expertise and experience in image interpretation (Heibel et al., 2020), which can limit accessibility to gold-standard screening services.
3. Real-World Effectiveness
In recent years, there has been an increase in the trial use of CNNs to aid in the identification and triage of several cancerous and non-cancerous skin conditions as a clinical decision support tool (CDS). Studies conducted into the efficacy of CNN in hospital and specialist dermatology environments provide evidence that CNNs perform better as a CDS for healthcare professionals rather than as a direct-to-consumer diagnostic tool. In more primary care settings (GPs and non-specialists) when used in tandem with clinical data, CNNs prove useful in determining and diagnosing skin lesions (exclusively when present in single instance indicative/suspicious lesions) from images. Furthermore, over a variety of studies, CNN models show superior, or at least equivalent, accuracy in comparison to clinicians, indicating future evolution of the models; however, it is prudent to recall that AI can often show false positives by misdiagnosing harmless lesions as malignant (Wong et al., 2022; Haggenmüller et al., 2021). In regard to specialist diagnoses, model accuracy for predicting malignant lesions was comparable to dermatologists (model: 71.31% vs. 3 dermatologists: 77.87%, 69.88% and 71.93%) (Wong et al., 2022). CNN models perform comparably to board-certified dermatologists; however, these must still be validated by larger datasets. CNN models use prior histopathological records and images as a ground truth for identification of skin lesions, while dermatologist consensus is more often used in real-world clinical settings with regards to clinical and family history and staging of progression of disease (Wong et al., 2022; Haggenmüller et al., 2021; Marsden et al., 2024).
Systematic reviews by Salinas et al. (2024) found that AI systems for skin cancer diagnosis achieved an overall sensitivity of 87.0% and specificity of 77.1%, compared with 79.8% sensitivity and 73.6% specificity for clinicians overall (Salinas et al., 2024). The differences were statistically significant (p < 0.001); however, when compared specifically with expert dermatologists, AI performance was clinically comparable rather than overtly superior, with sensitivities of 86.3% and 84.2% respectively (Salinas et al., 2024). The largest performance advantage was observed when AI was compared with generalist clinicians, where AI achieved a sensitivity of 92.5% compared with 64.6% for generalists. (Salinas et al., 2024). Overall, use of CNNs proves best in conjunction with primary/generalist needs – for use by general practitioners to improve accuracy and prioritise urgent cases, while remaining at roughly equal accuracy to expert dermatologists (Salinas et al., 2024).
CNNs achieve the highest diagnostic accuracy for common malignant and benign pigmented lesions, including malignant melanoma (Asare et al., 2025; Dhanalakshmi et al., 2025), basal cell carcinoma (Musthafa et al., 2024) and melanocytic nevi (common moles), which are well represented in training datasets (Musthafa et al., 2024; Kwiatkowska et al., 2021). Overall diagnostic accuracies for these lesion types often exceed 90% (Kommoss et al., 2026; Alamrani & Hujooj, 2026; Musthafa et al., 2024). In contrast, CNNs struggle to identify non-cancerous and rare lesions, including seborrheic keratosis and dermatofibroma (Kommoss et al., 2026), to identify rare skin tumours such as adnexal tumours and primary cutaneous lymphomas (Haggenmüller et al., 2021; Priyadarsini et al., 2026; Mazhar et al., 2023), and to distinguish atypical nevi from early-stage melanoma, resulting in reduced specificity and increased false-positive diagnoses (Kwiatkowska et al., 2021; Alshmrani et al., 2026; Agbarya et al., 2025). Overall, CNN performance remains highly dependent on the quality, diversity and representativeness of the training data, with underrepresented lesion types consistently demonstrating lower diagnostic accuracy. Holistically, the use of AI is only as good as its pre-input programming. It is subject to the same errors of its programmer, and while proving to be operationally accurate to an extent, it still requires further, conclusive validation from specialist dermatologists and cannot be held liable for its infrequent misdiagnoses.
From a clinician’s perspective, the integration of CNNs into dermatology offers a promising avenue for improving care pathways, especially in aid of GPs in primary care; these tools are approached as diagnostic aids rather than autonomous decision-makers (Nadour et al., 2025; Kwiatkowska et al., 2021). In time, the evolution of these systems into multimodal models – combining macroscopic images with comprehensive patient histories and genetic markers – could revolutionise triaging, possibly expanding the use to other skin lesions’ diagnostics, helping to catch aggressive melanomas earlier and manage swelling waiting lists within the NHS, where appointment wait times can exceed 90 days. In large-scale reader studies, a typical CNN can achieve a pooled sensitivity of 86% and a specificity of 94% for melanoma, matching or even outperforming junior dermatology trainees and general practitioners (Kwiatkowska et al., 2021; Yee et al., 2023; Heo & Shim, 2025). On the ward and in clinic, however, the practical implementation of CNNs introduces serious clinical risks, chief among them being the catastrophic potential for a false-negative result where a malignant lesion is misclassified as benign. Studies show that even top-performing architectures can miscategorise up to 28% of malignant melanomas as simple benign moles, directly delaying oncology referrals (Kommoss et al., 2026). Furthermore, because these algorithms are predominantly trained on a narrow spectrum of malignancies, there is a distinct danger that they will overlook or misinterpret severe, non-cancerous dermatological emergencies – such as erythroderma, toxic epidermal necrolysis or systemic autoimmune flare-ups – simply because the presentation falls outside their programmed parameters. This diagnostic tunnel vision is compounded by severe algorithmic bias; many models have been developed using images heavily weighted toward lighter skin types, meaning their diagnostic accuracy drops sharply for patients with skin of colour. As a result, diagnostic accuracy is lower in patients with skin of colour, increasing the risk of missed or delayed diagnoses. However, this narrow focus can also be a strength when the technology is used for a specific purpose. As a clinical decision support tool to help GPs assess suspicious skin lesions, CNNs can improve early cancer detection and support referral decisions. Problems arise when they are used as general diagnostic tools for all skin conditions rather than within their validated scope. Overreliance on these systems may provide false reassurance and delay the diagnosis of serious conditions that require urgent specialist assessment (Kommoss et al., 2026; Nadour et al., 2025; Yee et al., 2023; Heo & Shim, 2025). Real-world diagnostic trials confirm that standalone CNNs often underperform in everyday clinical practice, dropping to an overall diagnostic accuracy of just 56.7% when faced with rare or atypical presentations, failing to match expert dermatologists with over 10 years of experience who achieve 74.2% accuracy (Anriot et al., 2026). Ultimately, if consumer-facing apps bypass professional clinical oversight, they risk giving patients false reassurance or, conversely, critically risk misidentifying lesions. These factors are critical for the safe and effective adoption of AI-enabled skin cancer screening.
A major challenge when evaluating AI in dermatology is the variation between studies (e.g., differences in healthcare settings, clinician expertise, patient populations and disease categories assessed). Some studies compare AI systems with general practitioners, while others compare them with specialist dermatologists. In addition, studies may focus on different skin conditions, including melanoma, basal cell carcinoma, squamous cell carcinoma and non-neoplastic lesions, making direct comparisons difficult (Salinas et al., 2024).
The choice of a reference standard is also crucial. High-quality studies typically use histopathological confirmation from biopsies as the gold standard for diagnosis rather than visual assessment alone. This provides a more objective measure of whether an AI system correctly identifies malignant and benign lesions (Salinas et al., 2024).
Sensitivity and specificity are the most commonly reported outcome measures. In a systematic review and meta-analysis of 53 studies, Salinas et al. (2024) found that AI algorithms achieved an overall sensitivity of 87.0% and specificity of 77.1%, compared with 79.8% sensitivity and 73.6% specificity for clinicians overall. The authors reported statistically significant differences favouring AI. However, when AI systems were compared specifically with expert dermatologists, performance was clinically comparable rather than clearly superior. These findings suggest that AI may be particularly valuable in settings where specialist expertise is unavailable.
Despite promising accuracy results, researchers have highlighted concerns regarding real-world deployment. AI systems often perform well on curated datasets but may struggle when confronted with variations in image quality, lighting conditions, skin tones or uncommon diseases. Daneshjou et al. (2021) demonstrated substantial performance reductions when dermatology AI models were tested on diverse clinical images, particularly for darker skin tones. Similarly, Han et al. (2021) showed that image-based diagnostic models may lack robustness when applied in routine clinical environments.
Future developments are likely to focus on AI-assisted rather than AI-replacement models of care. Integrating CNN systems into clinical workflows could support healthcare professionals, especially non-specialists, in prioritising suspicious lesions, thereby reducing unnecessary biopsies and improving access to dermatological expertise while maintaining human oversight. Nevertheless, the risk of false negatives remains a significant concern, as missed skin cancers can have serious consequences for patient outcomes and guardrails to mitigate this risk are imperative.
4. Health Economics
Health economic analyses are used to evaluate the relative costs and outcomes of an intervention and determine whether it is cost-effective. Specific types of analyses include cost-minimisation (CMA), cost-benefit (CBA), cost-consequence (CCA), cost-effectiveness (CEA) and cost-utility (CUA) (Zilberberg et al., 2010). These analyses organise the available clinical and economic data and can help provide possible answers as to what intervention gives the greatest benefit proportional to its cost (Angevine et al., 2014). Regarding the implementation of AI for skin cancer detection, we will focus on CUA and CEA, which refer to analyses that examine the ratio of the cost of a particular intervention to a universal unit of effectiveness (Zilberberg et al., 2010). The CUA would use quality-adjusted life-years (QALYs) and CEA would use survival as a health outcome metric. Cost effectiveness studies, including CUA and CEA, inform effective resource allocation to maximise the net health benefit for a population derived from a fixed budget (Detsky et al., 1990). Cost-effectiveness studies conducted with QALYs can provide important information about a value-based price range for healthcare products and services. While there have been discussions that QALYs are discriminatory, for the purpose of this paper we will deem QALYs as a reasonable chosen unit of effectiveness (Willke et al., 2024) in addition to survival.
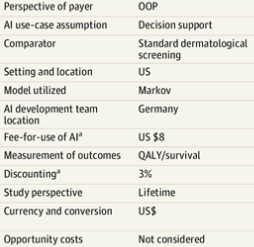
In implementing AI for skin cancer detection, a key consideration is cost-effectiveness. There is accumulating evidence that artificial intelligence can assist clinicians to make better clinical decisions. A more accurate assessment of suspicious skin lesions by GPs with AI assistance could lead to fewer onward referrals to dermatologists and unnecessary biopsies, reducing costs and improving patient outcomes (Jones et al., 2022), thereby enhancing quality of life (Grzybowski et al., 2024). However, a separate study performed using data and information from past papers has demonstrated contradictory results. Gomez Rossi et al. (2022) performed Monte Carlo microsimulations with 1000 random samples of people from the US, who would have AI to assist them in detection and diagnosis. The control group would then have normal physicians to observe and diagnose them (Gomez Rossi et al., 2022).
(Gomez Rossi et al., 2022)
The analysis was conducted from a payer perspective (Gomez Rossi et al., 2022). The results showed the mean costs were $750 for AI and $759 for dermatologists without AI, with similar mean health outcomes (AI: 86.6 QALYs; standard visual recognition: 86.6 QALYs) (Gomez Rossi et al., 2022). This has shown that AI may not have a big impact on cost reduction for a similar health outcome (Gomez Rossi et al., 2022). However, this paper had performed a simulation based on past results which may be outdated and only focused on the US, which implies that it may be inapplicable to other countries (Gomez Rossi et al., 2022). While there have been papers performing various cost-effectiveness studies for visual screening of skin cancer, there is a lack of health economic evidence for AI-enabled skin cancer screening.
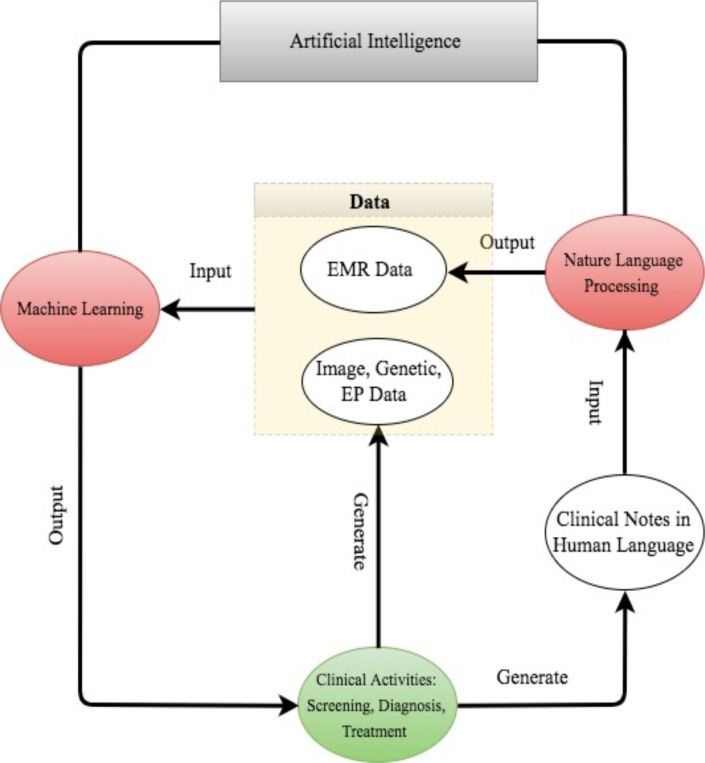
For AI to be used effectively for skin cancer detection, effort is needed from various parties. Healthcare teams should ensure that appropriate treatment pathways are in place after AI-assisted diagnosis to ensure maximum patient health benefits. Furthermore, AI developers need to work jointly with regulators and the medical community to make sure that new AI solutions are deployed where they best improve outcomes (Gomez Rossi et al., 2022). These parties must also ensure that the AI system is effective. A successful AI system must possess the machine learning component for handling structured data (images, EP data, genetic data) and the natural language processing component for mining unstructured texts.
(Jiang et al., 2017)
The sophisticated algorithms then need to be trained through healthcare data before the system can assist physicians with disease diagnosis (Jiang et al., 2017). Caution must be taken during development to avoid biases within the AI. It must be capable of identifying disease patterns and associations without a priori hypotheses – being unaffected by developer-introduced bias (Schwalbe et al., 2020). Effective implementation will also require understanding the local health system, as well as the social and epidemiological contexts (Wahl et al., 2018).
There are also existing limitations to current cost-effectiveness studies. One such limitation is that cost-effectiveness depends on the healthcare setting: the cost-effectiveness of AI implementation in skin cancer detection may provide greater benefits in some countries compared to others. Hence, the results of the health economic analyses in one country may be inapplicable to other countries (Diamond et al., 2009). Appropriate payment mechanisms must also be developed to incentivise new cost-effective therapies with this technology. The party who pays for the AI detection must be selected to ensure effective analysis (Gomez Rossi et al., 2022). Furthermore, the cost of AI could adversely affect the use, especially in resource-limited, rural and medically-underserved areas with limited access to dermatologic care (Beltrami et al., 2022). Aside from the sole economic quantitative aspects, the qualitative aspects of AI in healthcare for patients and society require further research (Wolff et al., 2020).
In summary, more research has to be done regarding the cost-effectiveness of the implementation of AI in skin cancer detection, taking multiple factors into consideration such as the various contexts in different countries.
5. Qualitative Implementation
In order to understand the public’s perspective on the integration of AI in the diagnostic pathway of skin cancer, a qualitative study was performed – a type of methodology which involves gathering an understanding of complex concepts and gathering deep insights (Lim, 2024). Qualitative research emphasises the context, existence, experience, perspective, meaning and subjectivity which allows researchers to explore and interpret the intricacy of social phenomena (Lim, 2024). Many researchers do qualitative studies for the ability to capture the richness of social phenomena involving human experiences and perspectives; these studies offer connections with real-world issues and respond rapidly to social changes (Lim, 2024). Using qualitative methodology, we can explore patients’ and healthcare professionals’ opinions on the usage of AI in the healthcare sector. The different methods of qualitative studies include interviews, focus groups (facilitated discussions with small groups of participants to explore shared experiences or perspectives), observations, case studies, ethnography (studying cultural practices and social norms through community immersion), document analysis and narrative research (Hassan, 2024).
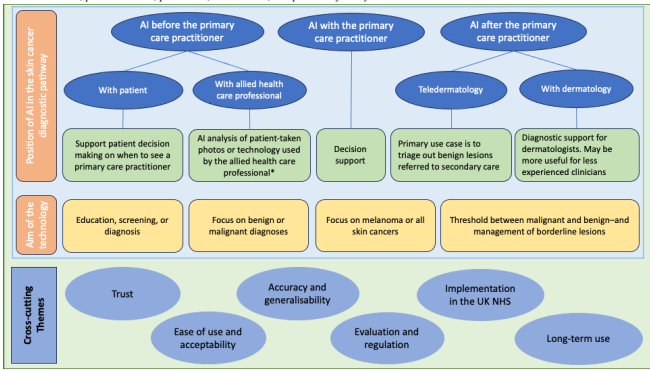
Since qualitative studies can be used to explore complex human experiences, a recent study was conducted where 29 stakeholders were questioned about the implementation and position of AI technologies in the skin cancer diagnostic pathway. The methodology used was a qualitative semi-structured interview study; these stakeholders were purposely sampled based on age, sex and geographical location (Jones et al., 2025). The interview was conducted using the Non-adoption, Abandonment, Scale-up, Spread and Sustainability (NASSS) framework which provides a comprehensive and accessible tool for evaluating and improving the implementation of healthcare innovations (Shin et al., 2025).
(Jones et al., 2025)
In this study, the majority of participants expressed their opinion of using AI before or with a primary care practitioner (PCP) to support patients in their decision of seeing a PCP or specialist (Jones et al., 2025). However, the minority of the participants who thought about the usage of AI after the PCP expressed how the implementation of AI at that stage can reduce the workload of PCPs and dermatologists, as well as improve consistency in their diagnosis (Jones et al., 2025). This can be successfully applied if the specialists are trained on how to interpret and diagnose successfully (Jones et al., 2025). Additionally, views of a higher body rather than individual GP practices (e.g., NHS on the adoption of AI technologies) are very important to gain the public’s trust.
Another key finding showed the accuracy of the technology has conflicting opinions according to AI researchers with academic and commercial backgrounds (Jones et al., 2025). Researchers with commercial backgrounds are in favour with the implementation of the technology whilst researchers with academic backgrounds were concerned about the accuracy of the technology, especially the diagnosis of skin cancers other than melanoma (Jones et al., 2025). These findings demonstrate the cultural influences on perceptions of AI, including values-based judgements informed by workplace experiences and attitudes.
In conclusion, the integration of AI in the diagnostic pathway for the detection of skin cancer, especially before or with a PCP is possible if the accuracy of the technology can be improved. This can be done by collecting data on people with “melanin-rich” skin and other forms of skin cancer other than melanoma (Jones et al., 2025) for adequate representation and robustness of diagnostic performance.
6. Bias and Ethical Considerations
The practice of healthcare revolves around a moral code which can be divided into four fundamental pillars of medical ethics (Ghimirie & Yadav, 2024). Medical ethics can be defined as principles that provide insight and guide medical personnel to have good judgement while practising medicine (Ghimirie & Yadav, 2024). These pillars are autonomy, beneficence, non-maleficence and justice, which are important when discussing the use of AI in healthcare such as detection of skin cancer (Ghimirie & Yadav, 2024).
The principle of beneficence can be defined as doing good to others where the professional is obligated (Kinsinger, 2010): to always and without exceptions favour the wellbeing and interest of the patient (Kinsinger, 2010). AI may breach beneficence in terms of diagnostic accuracy if it misses a diagnosis, depriving patients of necessary interventions such as excision of a lesion. Several studies by Nadour et al. (2025) and Shah and Agharwal (2026) demonstrate this. Out of 382 studies, only 38 met the inclusion criteria and out of the 38, 25 were found to have high risk of bias (Nadour et al., 2025). The study done by Shah and Raghaval (2026) showed that smartphone apps showed a mere 22% accuracy when analysing skin lesions (Shah & Agarwal, 2026). Another example comes from the Lancet where systematic reviews of many AI models were found to have a number of flaws. Out of 450 studies screened, only 20 met the inclusion criteria of bias evaluation. This bias was due to several factors such as AI models being trained on non-diverse populations (gender imbalance, income representation, geographic location etc.) (Singh et al., 2024; Combalia et al., 2022).
Non-maleficence is defined as “first, do no harm”. Under this, workers are to avoid acting with any intent to harm a patient and avoid providing treatments that are known to be ineffective or damaging (Ungvarsky, 2014). Due to low real-world diagnostic accuracy, the risk of false negatives when a lesion is identified as not malignant when it is (due to varied factors such as algorithmic bias) is significant. This poses risks as false negative results may provide false reassurances and may lead to delayed diagnoses and deprivation of life-saving treatment (Evans & Snead, 2024). With AI, there is also a risk of false positive results when AI flags a lesion as malignant although benign. When initial detection of skin cancer is found, patients undergo a step-by-step process of physical examination of skin including a biopsy, which is an invasive procedure, to remove a small sample of skin and cell samples. This can cause bleeding, infections and potential scarring which causes unnecessary harm to patients who are given a false positive result by AI – another potential breach of non-maleficence.
Autonomy is defined as the right and capacity of patients to govern their own healthcare, make informed decisions about their treatments and act as self-determining individuals (Varelius, 2006). For autonomy to be guaranteed, informed consent, total transparency and absence of coercion must happen. AI lacks this total transparency due its “black box” nature of outputs. The data at which AI gathers is random and sometimes unknown, which may also include biases (Pedreschi et al., 2019). This is referred to as the black-box phenomenon when a given input (information) produces an output (a response – in this case, whether a skin lesion is malignant or benign) without explanation or justification for the output given the inputs. This may limit patient autonomy as they are not able to understand why the AI has determined their lesion to be cancerous or not (Pedreschi et al., 2019). Therefore, doctors are not allowed to give informed consent if the decision process is unclear. Although certain studies show higher diagnostic accuracy than expert dermatologists, the data fails to show different groups (darker skin tones, different income population etc.). This further violates autonomy as patients are making decisions based on incomplete or misleading data whereby patients are not fully informed before giving consent (Combalia et al., 2022).
Justice is interpreted as the fair, equitable and appropriate treatment of people (Varkey, 2020). In terms of medical justice for AI in skin cancer screening, AI lacks distributive justice which refers to the fair equitable and appropriate distribution of healthcare resources. This is an ethical risk as more affluent populations will have greater access to AI such as apps that can detect skin cancer. In addition, digital exclusion may preclude certain populations less capable of using technologies, such as the elderly, thereby preventing them from accessing innovative care models. This causes a void at which higher-income and digitally-literate populations have access to supposedly “advanced” diagnostic aids as compared to lower-income or digitally-unskilled populations. AI also has algorithmic bias, which is when AI models produce unfair outcomes reflecting the limited data from which it was trained on. The accuracy of AI relies on the data at which the model has been trained, therefore if a dataset does not include a certain population, the AI model may underperform or misdiagnose this population.
7. Conclusion
AI, specifically CNNs, demonstrate high diagnostic accuracy for the detection of melanoma and non-melanoma skin cancers in controlled settings. Real-world studies reaffirm these findings; however, they are limited by a lack of representative cohorts with implications for validity and reliability amongst people with darker skin types. Furthermore, unexplainable AI outputs, coined the black-box phenomenon, limit the utility of such technology in skin cancer screening as it breaches the medical ethics pillar of autonomy and a patient’s right to self-determination regarding their healthcare. Economic considerations are critical for the adoption, scale-up and spread of AI-assisted skin cancer screening and there remains a paucity of evidence in this space. Future research should include ongoing real-world validation studies using representative populations and a range of skin types, with histopathological analysis as the gold standard, and comparing screening pathways (e.g., AI-assisted primary versus specialist care). Such studies may inform context-specific cost-effectiveness analyses crucial for sustainable financing of this technology.
Bibliography
Agbarya, A., Sabo, E., Sheikh-Ahmad, M., Saiegh, L., Pincas, M., Gorenberg, M., Shalata, W. & Faber, D.L. (2025) Malignancy in Ground-Glass Opacity Using Multivariate Regression and Deep Learning Models: A Proof-of-Concept Study, J Clin Med, 14(22):8082.
Alsaad, K.O., Obaidat, N.A. & Ghazarian, D. (2007) Skin adnexal neoplasms–part 1: an approach to tumours of the pilosebaceous unit, J Clin Pathol, 60(2), pp.129-44.
Angevine, P.D. & Berven, S. (2014) An Introduction to Cost-benefit, Cost-effectiveness, and Cost-utility Analyses, Spine, 39(22s), s9-s15.
Anriot, J., Yan, S., Coste, C. et al. (2026) Limits of artificial intelligence models for skin cancer diagnosis in realistic settings, JAMA Dermatol.
Arnold, M., Singh, D., Laversanne, M. et al. (2022) Global burden of cutaneous melanoma in 2020 and projections to 2040, JAMA Dermatology, 158(5), pp.495-503.
Asare, J.W., Kyei, E.A., Alornyo, S., Freeman, E., Ujakpa, M.M., Brown-Acquaye, W.L., Coleman, A. & Lempogo, F. (2025) Application of Medical Images for Melanoma Detection Using a Multi-Architecture Convolutional Neural Network From a Deep Learning Approach, Engineering Reports, 7: e70096.
Beltrami, E.J., Brown, A.C., Salmon, P.J.M. et al. (2022) Artificial intelligence in the detection of skin cancer, Journal of the American Academy of Dermatology, 87(6), pp. 1336-1342.
Brinker, T.J., Hekler, A., Utikal, J.S., Grabe, N., Schadendorf, D., Klode, J., Berking, C., Steeb, T., Enk, A.H. & von Kalle, C. Skin (2018) Cancer Classification Using Convolutional Neural Networks: Systematic Review, J Med Internet Res, 20(10):e11936.
Carli, P., De Giorgi, V., Salvini, C., Mannone, F. & Chiarugi, A. (2002). The gold standard for photographing pigmented skin lesions for diagnostic purposes: contact versus distant imaging, Skin Research and Technology, 8(4), pp.255-259.
Combalia, M., Codella, N., Rotemberg, V., et al. (2022). Validation of artificial intelligence prediction models for skin cancer diagnosis using dermoscopy images: the 2019 International Skin Imaging Collaboration Grand Challenge, The Lancet Digital Health, 4, e330-e339.
Daneshjou, R., Vodrahalli, K., Liang, W. et al. (2021) Disparities in Dermatology AI: Assessments Using Diverse Clinical Images, arXiv: 2111.08006.
Detsky, A.S. & Naglie, I.G. (1990) A Clinician’s Guide to Cost-Effectiveness Analysis, Annals of Internal Medicine, 113(2), pp. 147-154.
Dhanalakshmi, K., Kumar, S., Mishra, S., Susitra, D., Lalitha, R. & Dharani, V. (2025) Classification of Benign and Malignant Skin Lesions using Convolutional Neural Networks (CNN), 2025 International Conference on Intelligent Computing and Control Systems, pp. 792-798.
Diamond, G.A. & Kaul, S. (2009) Cost, effectiveness, and cost-effectiveness, Circulation: Cardiovascular Quality and Outcomes, 2(1), pp.49-54.
Eriksson, T. & Tinghög, G. (2014) Societal cost of skin cancer in Sweden in 2011, Acta Dermato-Venereologica, 95(3), pp.347–348.
Esteva, A., Kuprel, B., Novoa, R.A. et al. (2017) Dermatologist-level classification of skin cancer with deep neural networks, Nature, 542(7639), pp. 115–118.
Evans, H. & Snead, D. (2024) Understanding the errors made by artificial intelligence algorithms in histopathology in terms of patient impact, NPJ digital medicine, 7(1), 89.
Fan, J., Ma, C. & Zhong, Y. (2021) A selective overview of deep learning, Statistical Science, 36(2), pp.264-290.
Ghimire, N. & Yadav, D. (2024) Touch of Medical Ethics at the Beginning of Medical School, Journal of the Nepal Medical Association, 62(273), pp. 350-352.
Gomez Rossi, J., Rojas-Perilla, N., Krois, J., Schwendicke, F. et al (2022) Cost-effectiveness of Artificial Intelligence as a Decision-Support System Applied to the Detection and Grading of Melanoma, Dental Caries, and Diabetic Retinopathy, JAMA Network Open, 5(3), e220-e269.
Grzybowski, A., Jin, K. & Wu, H. (2024) Challenges of artificial intelligence in medicine and dermatology, Clinics in Dermatology, 42(3), pp.210-215.
Gurumurthy, R., Mohapatra, R.K., Easow, J.M. & Mohan, S. (2015) Cutaneous B cell lymphomas: Report of two interesting cases, Indian J Dermatol, 60(2), pp.176-178.
Haenssle, H.A., Fink, C., Schneiderbauer, R. et al. (2018) Man against machine: diagnostic performance of a deep learning convolutional neural network for dermoscopic melanoma recognition in comparison to 58 dermatologists, Annals of Oncology, 29(8), pp.1836-1842.
Haggenmüller, S., Maron, R., Hekler, A. et al. (2021) Skin cancer classification via convolutional neural networks: systematic review of studies involving human experts, European Journal of Cancer, 156, pp.202-216.
Hasan, N., Nadaf, A., Imran, M. et al. (2023) Skin cancer: understanding the journey of transformation from conventional to advanced treatment approaches, Molecular Cancer, 22(168).
Hassan, M. (2026) Qualitative Research – Methods, Analysis Types and Guide, Research Method [online]. <https://researchmethod.net/qualitative-research/>
Heibel, H., Hooey, L. & Cockerell, C. (2020) A Review of Noninvasive Techniques for Skin Cancer Detection in Dermatology, American Journal of Clinical Dermatology, 21(4), pp.515-524.
Heo, E.J. & Shim, J.B. (2026) Minimizing the False Negative Rate in Convolutional Neural Network-Based Melanoma Classification Using Hyperspectral Data to Reduce Misdiagnosis, Prog. Med. Phys, 37, pp.19-27.
Istasy, P., Lee, W.S., Iansavichene, A., Upshur, R., Gyawali, B., Burkell, J., Sadikovic, B., Lazo-Langner, A. & Chin-Yee, B. (2022) The Impact of Artificial Intelligence on Health Equity in Oncology: Scoping Review, Journal of medical internet research, 24(11), e39748.
Jiang, F., Jiang, Y., Zhi, H., Dong, Y., Li, H., Ma, S., Wang, Y., Dong, Q., Shen, H., Wang, Y (2017) Artificial intelligence in healthcare: past, present and future, Stroke Vasc Neurol, 2(4), pp.230-243.
Jones, O.T., Calanzani, N., Scott, S.E., Matin, R.N., Emery, J. & Walter, F.M. (2025) User and Developer Views on Using AI Technologies to Facilitate the Early Detection of Skin Cancers in Primary Care Settings: Qualitative Semistructured Interview Study, JMIR Cancer, 11, e60653.
Jones, O., Matin, R., van der Schaar, M., Prathivadi Bhayankaram, K., Ranmuthu, C., Islam, M., Behiyat, D., Boscott, R., Calanzani, N., Emery, J., Williams, H. & Walter, F. (2022) Artificial intelligence and machine learning algorithms for early detection of skin cancer in community and primary care settings: a systematic review, The Lancet Digital Health, 4(6), e466-e467.
Kinsinger, F. S. (2009) Beneficence and the professional’s moral imperative, Journal of chiropractic humanities, 16(1), pp.44-46.
Kocarnik, J.M., Compton, K., Dean, F.E. et al. (2022) Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the Global Burden of Disease Study 2019, JAMA Oncology, 8(3), pp.420-444.
Kommoss, K.S., Winkler, J.K., Vollmer, A.S. et al. (2026) Multiclass convolutional neural network vs. 96 dermatologists in skin lesion diagnosis, an international study, Journal der Deutschen Dermatologischen Gesellschaft, 1-9.
Kwiatkowska, D., Kluska, P. & Reich, A. (2021) Convolutional neural networks for the detection of malignant melanoma in dermoscopy images, Postepy Dermatol Alergol, 38(3), pp.412-420.
Lim, W.M. (2024) What Is Qualitative Research? An Overview and Guidelines, Australasian Marketing Journal, 33(2), pp.199-229.
Marsden, H., Kemos, P., Venzi, M., Noy, M., Maheswaran, S., Francis, N., Hyde, C., Mullarkey, D., Kalsi, D. & Thomas, L. (2024) Accuracy of an artificial intelligence as a medical device as part of a UK-based skin cancer teledermatology service, Front Med (Lausanne), 11:1302363.
Mittelstadt, B. (2019) Principles alone cannot guarantee ethical AI, Nat Mach Intell, 1, pp.501-507.
Musthafa, M.M., Mahesh, T.R., Vinoth Kumar, V., & Guluwadi, S. (2024) Enhanced skin cancer diagnosis using optimized CNN architecture and checkpoints for automated dermatological lesion classification, BMC Med Imaging, 24(1):201.
Nadour, N., Duguet, T., Zahedi, S., Figoni, H. & Liard, R. (2025) Diagnostic accuracy of artificial intelligence compared to family physicians and dermatologists for skin conditions: a systematic review and meta-analysis, BMC Prim Care, 26(1):384.
Nagarajan, P., Asgari, M.M., Green, A.C. et al. (2019) Keratinocyte carcinomas: current concepts and future research priorities, Clinical Cancer Research, 25(8), pp.2379-2391.
Obermeyer, Z., Powers, B., Vogeli, C. & Mullainathan, S. (2019). Dissecting racial bias in an algorithm used to manage the health of populations, Science (New York, N.Y.), 366(6464), pp.447-453.
Papachristou, P. et al. (2024) Evaluation of an artificial intelligence-based decision support for detection of cutaneous melanoma in primary care – a prospective, real-life, clinical trial, British Journal of Dermatology, 191(1).
Pedreschi, D., Giannotti, F., Guidotti, R., Monreale, A., Ruggieri, S. & Turini, F. (2019) Meaningful Explanations of Black Box AI Decision Systems, Proceedings of the AAAI Conference on Artificial Intelligence, 33(01), pp.9780-9784.
Priyadarsini, R.N., Tyagi, B. & Priyadharsini, M. (2026) An attention based optimized network for the classification of skin lesions, Sci Rep, 16(1):3494.
Purwono, P., Ma’arif, A., Rahmaniar, W. et al. (2022) Understanding of Convolutional Neural Network (CNN): a review, International Journal of Robotics and Control Systems, 2(4), pp.739-748.
Roky, A.H., Islam, M.M., Ahasan, A.M.F. et al. (2025) Overview of skin cancer types and prevalence rates across continents, Cancer Pathogenesis and Therapy, 3(2), pp.89-100.
Salinas, M.P., Sepúlveda, J., Hidalgo, L., Peirano, D., Morel, M., Uribe, P., Rotemberg, V., Briones, J., Mery, D. & Navarrete-Dechent, C. (2024) A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis, npj Digital Medicine, 7(1).
Schwalbe, N., Wahl, B. et al. (2020) Artificial intelligence and the future of global health, Lancet, 395(10236), pp.1579-1586.
Shah, A.K. & Agarwal, M. (2026) Diagnostic Accuracy of Artificial Intelligence Applications on a Diverse Skin Image Set, Cureus, 18(1):e102354.
Shin, H.D., Hamovitch, E., Gatov, E., MacKinnon, M., Samawi, L., Boateng, R., Thorpe, K.E. & Barwick, M. (2025) The NASSS (Non-Adoption, Abandonment, Scale-Up, Spread and Sustainability) framework use over time: A scoping review, PLOS Digital Health, 4(3), e0000418.
Singh, Y., Patel, H., Vera-Garcia, D.V., Hathaway, Q.A., Sarkar, D. & Quaia, E. (2024) Beyond the hype: Navigating bias in AI-driven cancer detection, Oncotarget, 15, pp.764-766.
Stajic, J., Stone, R., Chin, G. & Wible, B. (2015) Rise of the Machines, Science, 349(6245), pp.248-249.
Tschandl, P., Rosendahl, C. & Kittler, H. (2018) The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions, Scientific Data, 5(180161).
Varelius J. (2006) The value of autonomy in medical ethics, Medicine, health care, and philosophy, 9(3), pp.377-388.
Varkey, B. (2021) Principles of Clinical Ethics and Their Application to Practice, Medical principles and practice : international journal of the Kuwait University, Health Science Centre, 30(1), pp.17-28.
Wahl, B., Cossy-Gantner, A., Germann, S., Schwalbe, N.R. et al. (2018) Artificial intelligence (AI) and global health: how can AI contribute to health in resource-poor settings?, BMJ Global Health, 3(4), e000798.
Wei, M.L., Tada, M., So, A. & Torres, R. (2024) Artificial intelligence and skin cancer, Frontiers in medicine, 11, 1331895.
Willke, R., Pizzi, L., Rand, L., Neumann, P. et al. (2024) The Value of the Quality-Adjusted Life Years, Value in Health, 27(6), pp.702-705.
Wolff, J., Pauling, J., Keck, A. & Baumbach, J. (2020) The Economic Impact of Artificial Intelligence in Health Care: Systematic Review, Journal of Medical Internet Research, 22(2), e16866.
Wong, S.C., Ratliff, W., Xia, M. et al. (2022) Use of Convolutional Neural Networks in Skin Lesion Analysis Using Real World Image and Non-Image Data, Frontiers in Medicine, 9, 946937.
Yee, J., Rosendahl, C. & Aoude, L.G. (2024) The role of artificial intelligence and convolutional neural networks in the management of melanoma: a clinical, pathological, and radiological perspective, Melanoma Res, 34(2), pp.96-104.
Young, A.T., Fernandez, K., Pfau, J. et al. (2021) Stress testing reveals gaps in clinic readiness of image-based diagnostic artificial intelligence models, npj Digital Medicine, 4(10).
Zilberberg, M., Shorr, A. et al. (2010) Understanding cost-effectiveness, Clinical Microbiology and Infection, 16(12), pp.1707-1712.




{kind=link}