
Supervised by: Chi Him Kendrick Yiu BSc (Hons), MRes. Kendrick is studying for a DPhil in Medical Sciences at Wolfson College, University of Oxford, specialising in cardiovascular research. He graduated with a Bachelor’s Degree in Biomedical Sciences in Hong Kong before pursuing a Master’s Degree in Clinical Research at Imperial College London. His interests lie in the mechanisms of heart diseases and their potential therapies.
Abstract
This paper examines how the practice of cardiology is transforming with the rapid advancements in artificial intelligence (AI). This review offers an in-depth analysis of recent advancements in the risk stratification, diagnosis and surgery using AI with regard to the major cause of cardiology death, coronary artery disease (CAD). In order to determine if AI will permanently have a role in the field of cardiology for the best possible patient health and care, this paper analyzes the previous treatment of CAD and the future AI-assisted strategies for treating CAD.
1. Introduction
Coronary artery disease (CAD) is one of the world’s leading causes of death, accounting for 17.8 million deaths annually (Brown, Gerhardt and Kwon 2023). If untreated, CAD can result in heart attack, leading to hospitalization and permanent damage to the heart muscle. Moreover, with today’s rapidly growing population, it is predicted that CAD rates will increase by 31% by 2060 (OSF, 2022). In order to halt this disease’s mortality rates, it is crucial to transform the way we manage it. The use of artificial intelligence (AI) in medicine has been experiencing a tremendous breakthrough in recent years, with more studies being published than ever before. While most areas of medicine have embraced AI, cardiology has utilized it more than most. According to the FDA’s update in January 2023, there are 58 FDA-cleared algorithms across the speciality of cardiology, second only to radiology which has 396 (Cardiovascular Business, 2023). From diagnosing CAD to assisting in surgery, AI is capable of revolutionizing the way CAD is treated. In this review paper, we discuss the different ways AI can reduce the mortality rates of CAD.
2. Coronary Artery Disease
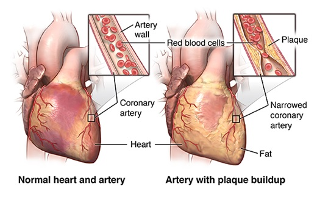
Coronary artery disease (CAD) is a heart disease caused by a build-up of plaque in the artery walls (Centers For Disease Control and Prevention, 2021). The coronary arteries supply blood to the heart and other parts of the body. The plaque is made up of cholesterol and other substances in the artery; the plaque build-up causes the arteries to narrow over time and block the flow of blood. This process is called atherosclerosis (Centers for Disease Control and Prevention, 2021). People with coronary artery disease may not realize that something is wrong until plaque causes blood clots. CAD can occur for many years asymptomatic until the person experiences a heart attack. This is when your heart muscle starts to die because it is not receiving enough blood.
The two main forms of CAD are stable ischemic heart disease and acute coronary syndrome. Stable ischemic heart disease (chronic CAD) is when the coronary arteries narrow gradually over years. The heart receives less oxygenated blood and the person can survive for many years while experiencing symptoms. Acute coronary syndrome is when the plaque in the coronary artery ruptures and forms a blood clot that blocks the flow of blood to the heart. This causes a heart attack. CAD can weaken your heart and lead to the following complications: arrhythmias, cardiac arrest, cardiogenic shock, and heart failure (Cleveland Clinic, 2023).
3. Medication treatments of CAD
CAD has been the leading cause of death in the USA since 1950 as a result of the development of vaccines against viral and bacterial diseases such as tuberculosis (Heron, Aderson, 2016). This long predates the use of AI in aiding practitioners to diagnose, treat and monitor patients. Before AI and machine learning were seen as commonplace in a clinical setting, more traditional methods (methods that were less heavily reliant on machines and modern technology) were used and are still used today.
During patient diagnosis for CAD, a practitioner will often begin with a blood test. This will not only be useful in terms of heart monitoring but will also give a generalized overview of the patient’s health. Other diagnostic tests may include ECG, coronary angiography, and MRI scans. These methods are often used in place of methods that use AI for various reasons. For example, a coronary angiography costs the UK’s National Health Service (NHS) £1,300 (BBC News, 2010). This procedure involves a catheter being inserted into a blood vessel in the groin or arm (a local anesthetic is commonly used in this procedure.) The catheter is then fed to the coronary arteries via the aid of x-ray images. A contrast medium is then injected through the catheter and the angiogram is taken (NHS, 2022). The contrast medium is then visible on the angiogram and practitioners can visibly see where the arteries have become blocked and to what extent.
CAD can be treated in a variety of ways and become tailored to the specific circumstances of individual patients. From the 1960s/1970s, invasive and complex surgeries (such as coronary artery bypass surgery) became more frequent; in the 1980s, stents were used to prop open arteries (Healthline, 2018). However, less invasive approaches, such as prescribing medication, can also be used. Blood-thinning medicines can reduce the risk of cardiac arrest by thinning the blood and reducing the chance of blood clots forming. If a patient suffers from atrial fibrillation, the use of an anticoagulant may reduce their risk of taking a stroke by up to 60% (Healthline, 2023). Common blood-thinning medicines may include low-dose aspirin, clopidogrel, rivaroxaban, ticagrelor or prasugrel.
i. Statins
High blood cholesterol levels in patients is a heavily contributing factor if CAD is to arise. In order to combat this without the use of AI, practitioners may prescribe statins. Statins used by the British NHS may include atorvastatin, simvastatin, rosuvastatin or pravastatin (NHS, 2020). Medications such as these decrease blood cholesterol levels by increasing the number of low-density lipoprotein (LDL) receptors in the liver and preventing the formation of cholesterol (NHS, 2020). This helps remove LDL from the blood which makes the occurrence of a cardiac arrest less likely. Not all statins are suitable or effective for all patients, so several may need to be taken in order to determine which is most effective.
ii. ACE inhibitors
Angiotensin-converting enzyme (ACE) inhibitors, such as ramipril or lisinopril, are commonly used to treat high blood pressure. They work by inhibiting the hormone, angiotensin-2. When taking ACE inhibitors, a patient’s blood pressure will likely be monitored, and regular blood tests are taken to monitor kidney function. However, less than 1 in 100 people suffer from renal stenosis as a result of taking ACE inhibitors (NHS, 2020). Alternatively, angiotensin-2 receptor blockers (ARBs) may be offered to patients. Similarly, to ACE inhibitors, ARBs also inhibit angiotensin-2 and may be used in preference to ACE inhibitors as their only common side effect is mild dizziness (ACE inhibitors may cause a dry cough in some cases) (NHS, 2020).
iii. Nitrates
During treatment for angina, nitrates may be administered to a patient. This particular medication causes vasodilation by donating nitric oxide (NO) (National Library of Medicine, 2023). Nitrates become effective when activated by mitochondrial or ALDH2 into NO, which is an endothelium-derived relaxing factor (Daiber & Munzel, 2015). NO is produced by the endothelium to dilate blood vessels, however diseases such as atherosclerosis may reduce NO levels (Daiber & Munzel, 2015). NO has the ability to activate soluble guanylate cyclase which causes an increase of intracellular cGMP and its dependent protein kinases, such as cGK-I. cGK-I inhibits inositol-1,4,5-trisphosphate-dependent calcium release (Daiber, & Munzel, 2015). Smooth muscle relaxation is achieved as un-phosphorylated myosin light chain causes the myosin head to detach from actin. As intracellular calcium levels have decreased, this has a knock-on effect and inhibits myosin light chain kinase (Daiber & Munzel, 2015). The resulting venodilation allows blood to flow smoother and more easily through blood vessels including the coronary arteries. This allows the heart to work with less stress and at a lower rate, which decreases heart oxygen demands for aerobic respiration to allow the myogenic muscle to contract. Venodilation increases the venous capacitance and lowers the preload; this subsequently lowers the left ventricular end-diastolic pressure (National Library of Medicine, 2023).
4. Artificial Intelligence in Medicine
The use of machinery to search medical data and discovery aid in improving health outcomes and patient experiences. AI uses computers and technology to simulate behavior and critical thinking similar to a human being. There are two different applications of AI: virtual and physical. The virtual part of AI manages applications such as electronic health records and neural network based guidance in treatment decisions. The physical application of AI deals with robots assisting in surgeries, prostheses for handicapped people, and elderly care (National Library of Medicine, 2015).
i. Machine Learning
Machine learning is a branch of AI that uses data and algorithms to imitate the way people learn. There are three main parts in which a machine learning algorithm works (IBM, 2023). The first part is a “decision process”, where the algorithm can make a prediction or classification based on inputted data that is either labeled or unlabeled. The second part is an “error function”. This evaluates the prediction of the model by making a comparison with known examples to test the accuracy of the model. The third part is a “model optimization process”, whereby if the model can have a better fit for the data points in the training set, then weights are adjusted to lower any inconsistency between the known example and model estimate (IBM, 2023). The model will repeat this process continuously until it reaches a certain level of accuracy (IBM, 2023).
ii. Deep Learning
Deep learning is a more advanced field of machine learning to solve more complex problems (Edureka, 2023). Deep learning models learn to focus on the right feature by themselves with less guidance. Deep learning is able to mimic the functions of our brain by using artificial neurons, which function the same as biological neurons in our brain. It is able to find out the features important for classification using deep neural networks. Deep learning works on different levels. At the lowest level, the network focuses on patterns of local contrast. The next layer uses those patterns to identify more complex figures, such as eyes, noses, and mouths. Then, the top layer can finally apply those facial features to face templates (Edureka, 2023). Convolutional Neural Network is a type of neural network consisting of three main layers; convolutional, pooling and fully connected layers. Each layer then has a specific amount of sub-layers varying on the type of CNN.
Machine learning and deep learning differ in the type of data they work with and the methods in which they learn. Machine learning algorithms use structured, labeled data to make predictions. They take specific features that are defined from the input data for the model so that it can be organized into tables. Deep learning doesn’t require pre-processed data. Instead the algorithms can process unstructured data and automate feature extraction without the need for human experts (IBM, 2023). Machine learning and deep learning focus on supervised, unsupervised, and reinforcement learning. Supervised learning uses labeled datasets to categorize or make predictions. Unsupervised learning doesn’t require labeled datasets but detects patterns in the data and clusters by any distinguishable characteristics. Finally, reinforcement learning is when a model becomes more accurate for performing an action based on the feedback given (IBM, 2023).
5. AI-assisted Risk Stratification of CAD
i. Coronary Artery Calcium
Coronary artery calcium score (CAC) is a value that measures the amount of calcified plaque in the coronary arteries. It is used to quantify coronary atherosclerosis and is a meaningful predictor of CAD, as well as myocardial infarction. This is an especially useful technique as it can evaluate how hindered the blood flow in the heart is, thus approximating the risk of CAD (Heart Foundation). Nevertheless, CAC scoring requires an expert and is labor-intensive (Lin, 2021). Therefore, there have been studies assessing whether an artificial intelligence-based algorithm could take over this task. A study by Lessmann et al. (2018) presented a method for an automatic detection of coronary artery calcifications on chest CT scans. The researchers developed a convolutional neural network (CNN), a type of deep learning that specializes in computer recognition of grid-like structures, such as images. This study used two consecutive convolutional neural networks, training them with a set of 1744 CT scans. The first CNN is responsible for identifying possible calcifications based on the location and appearance. This is achieved by distinguishing all of the voxels (data points in a grid, such as image) in the CT scan that have a density higher than 130 Hounsfield units (HU) (Lessmann et al., 2018). HU is a unit measuring the presence of calcification by its density. The larger the HU, the denser the area, meaning the severer the calcification (Gücük and Üyetürk, 2014). Nevertheless, in order to increase the precision of this algorithm, a second CNN is needed. This is on account of different circumstances, such as metal artifacts, background noise, and highly dense structures in the body lead to false positive classifications of calcification. Therefore, the second convolutional neural network takes the results of the first CNN and differentiates between true and false calcifications by focusing on more hidden and precise details (Lessmann et al., 2018). Utilizing this method of CAC scoring can expedite the process and offer more patients with the opportunity for CAD risk stratification. If in the future this method is refined and implemented in hospitals, it would very likely have a meaningful impact on preventing CAD mortality.
6. AI-assisted Diagnosis of CAD
i. Echocardiography
Echocardiography is one of the most accessible and commonly used diagnostic instruments in cardiology. Echocardiography has been used to produce images of the heart’s structure since 1880 (Maleki and Esmaeilzadeh, 2012). However, echocardiography interpretation is not only time-consuming, it is and continues to become increasingly complex with new advancements in the field. Therefore, it requires specialists in echo examinations in cardiology. Unfortunately, in some countries there is a lack of trained cardiologists conducting echocardiography and their labor is often overtaken by ultrasound specialists, who are not entirely familiar with the field (Yu, 2017). Using AI in echocardiogram interpretation is a reasonably new idea that has yet to be further developed, nevertheless has been subject of several studies. An example is a study from 2018, at the University of California, that trained a CNN to classify 15 different views of an echocardiogram. Views are the different angles at which heart images are produced. The goal of this study was to determine whether AI was able to recognize the different views produced by an electrocardiogram, which is one of the first steps of interpretation. Twelve of the views were videos, and three were still images. The computer was given 200,000 images and videos, all of different patients with a range of heart conditions, and was trained to classify them according to what heart anatomy was shown in the image or video. The twelve video views were successfully classified with an accuracy of 98%. The still images on the other hand had a slightly lower accuracy of 92%, but was higher than the 80% accuracy accomplished by a team of four professional echocardiographers (Madani, Aranout and Mofrad, 2018). By using AI in the first step of interpreting an echocardiogram image, physicians save time, and misinterpretation is prevented. This is one example of how AI has already been introduced to the subject of echocardiography.
ii. Electrocardiography
The following step to using AI interpretation is in diagnosis, with the majority of studies found being those on electrocardiography (EKG). By using deep-learning algorithms, AI is able to diagnose patients merely by analyzing EKG tests. This works by giving the algorithm millions of previous EKG tests and the corresponding patient outcomes. The computer then finds patterns and corresponds them to certain outcomes. As mentioned in section 3.2 of this report, this concept of AI is referred to as supervised learning. Thus the AI learns to detect specific patterns in echocardiograms and associate them with a specific diagnosis. By analyzing and learning copious amounts and sets of patterns in the EKG images, the machine can detect and learn the most indistinct patterns which conceivably pass unseen by the human eye (Powerful Medical, 2023). In other words, the algorithm teaches itself how to interpret ECG images. In the case of CAD, the computer will be looking for abnormalities in the ECG images, most commonly being abnormally high T-waves and long QT intervals, which are caused by CAD. However, elevated or depressed ST-segments are also a sign of CAD (Medical News Today, 2022).
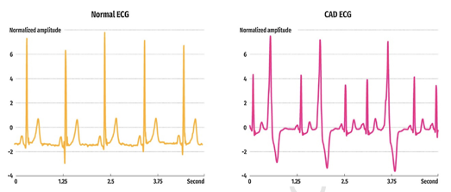
Figure 1: An example of a normal and CAD 5-s ECG segment (Archaya et al., 2018).
In this figure, it is visible how the CAD ECG illustrates very high T-waves and longer QT intervals, than the normal ECG.
A study by Archaya developed a convolutional neural network (CNN) that detects between normal and CAD ECG (five seconds) with an accuracy of 95.11%. This study developed an eleven-layered CNN that is considered easy to operate and highly cost-effective. Such CNN can help clinicians accurately diagnose CAD and simultaneously make ECG interpretation proceed much faster, allowing an increase in ECG appointments for patients (Archaya et al., 2017).
ii. Coronary Computed Tomographic Angiography
Coronary computed tomographic angiography (CCTA) is a non-invasive diagnostic test that produces three-dimensional (3D) images of the coronary arteries. It is used to assess the coronary arteries and detect abnormalities, such as atherosclerosis. A contrast dye is injected into the blood vessels and a series of X-ray images are taken from numerous angles with which a computer program produces 3D images of the coronary arteries (Hopkins Medicine). A high-quality visual assessment is crucial in understanding and interpreting CT images. However, similar to ECG, the interpretation is time-consuming and requires well-trained professionals. A study by the Journal of Medical Imaging developed a support vector machine learning algorithm combined with a formula-based analytic method to detect obstructive and non-obstructive stenosis. They used geometric and shape features of coronary lesions as inputted data. The algorithm was able to detect obstructive from non-obstructive stenosis with an accuracy of 94% (Kang et al., 2015).
7. CAD Surgeries
i. History and Importance
The history of CAD surgery exemplifies the ceaseless quest for innovative treatments. In the mid-20th century, a significant development in CAD surgery emerged before the widespread adoption of coronary artery bypass grafting (CABG). Dr. Rene Favaloro, an Argentinean surgeon, etched his name in history with one of the inaugural CABG surgeries in 1967. He ingeniously utilized a vein transplant to bypass a blocked coronary artery, offering a lifeline to those with formidable coronary artery blockages and dramatically shifting the landscape of CAD surgery. Pre-CABG, percutaneous transluminal coronary angioplasty (PTCA), pioneered by Dr. Andreas Gruentzig in the late 1970s, represented a major intervention. PTCA involved inflating a balloon within a constricted artery to restore blood flow, though it had limitations for complex CAD cases. The introduction of stent technology in the 1980s, coupled with the evolution of minimally invasive techniques like percutaneous coronary intervention (PCI) and minimally invasive direct coronary artery bypass (MIDCAB), has continued to revolutionize CAD surgery, resulting in vastly improved patient outcomes and post-surgery quality of life. This history underscores the pivotal role surgical innovations have played in advancing the treatment of CAD, one of the most prevalent cardiovascular conditions (European Heart Journal, 2013).
ii. Traditional Open-Heart Surgeries
Traditional open-heart surgery, also known as cardiac surgery, involves an incision around roughly 6-8 inches, often in the middle of the chest, to access the heart. A heart-lung bypass system temporarily replaces the heart’s ability to pump blood during the procedure, enabling surgeons to replace or repair heart valves, cure congenital abnormalities, or implant ventricular assist devices (VADs) and total artificial hearts (TAHs). The heart is restarted, and the chest is sutured shut after all necessary interventions have been carried out. While traditional open-heart surgery has a 1-year-post-op survival rate of roughly 96-97% , it is being supplemented in some situations by minimally invasive procedures that may result in quicker recovery times and less trauma (Medical News Today, 2018). The patient’s condition, age, and general health all have a role in the surgical method that is chosen.
a. Coronary Artery Bypass Graft Surgery (CABG)
One of the most popular open-heart surgical procedures, CABG, is used to treat severe CAD. When CAD has drastically decreased blood supply to the heart muscle and symptoms like angina (chest pain caused by reduced blood flow to the heart muscles) or a high risk of heart attack is present, CABG is frequently advised. To access the heart during CABG, a surgeon creates an incision in the chest, frequently by a median sternotomy (procedure done to separate your sternum (breastbone)). A heart-lung bypass machine momentarily stops the heart and takes over the job of pumping blood, allowing it to be diverted away from the heart. A healthy blood vessel is then taken from the patient’s leg (saphenous vein) or chest (internal mammary artery). By opening a new route, blood may flow directly to the heart muscle without being blocked, restoring oxygen and nutrition supply. If necessary, multiple grafts can be applied simultaneously. Regarding treating angina, enhancing general heart health, and lowering the risk of heart attacks, CABG has been demonstrated to be beneficial. Following CABG, survival rates are often very high, and most patients report significant symptom reduction and improved quality of life. Long-term results are positive, and many patients have increased longevity and heart health. Individual results, however, may differ depending on the patient’s demographics, the severity of their CAD, and the existence of other medical disorders. It’s crucial to note that CABG is a significant surgery with inherent risks, such as those related with anesthesia, infection, and postoperative complications. After a thorough examination by a cardiovascular specialist and a detailed comparison of the advantages and potential hazards, the decision to undertake a CABG is reached. The safety and efficacy of CABG have steadily increased with developments in surgical procedures and postoperative care, making it an essential and well-recognized intervention in the therapy of CAD (NHS, 2021).
b. Off-Pump Coronary Artery Bypass (OPCAB)
Off-pump coronary artery bypass (OPCAB) surgery is a specific type of open-heart surgery that is carried out without using a heart-lung bypass machine, which is an important component of conventional CABG. When the coronary arteries are severely constricted or obstructed, reducing blood flow to the heart muscle, OPCAB is often carried out for the same reasons as CABG. OPCAB involves the surgeon making a chest incision through which the heart is visible. The surgeon uses specialized instruments and methods to stabilize and immobilize the portion of the heart where the grafts will be put rather than halting the heart and utilizing a heart-lung machine. As a result, the surgery can be done while the heart is still beating. Grafts are then carefully joined to the coronary arteries beyond the obstructions, forming new blood flow routes, and are frequently taken from the patient’s own arteries or veins. The purpose of OPCAB is to lessen the hazards that could arise from using a heart-lung bypass system, such as bleeding, inflammation, and blood component damage. OPCAB may result in quicker recuperation times, fewer problems, and possibly better outcomes for some patients by avoiding the usage of the machine. Following 3-year post-operation, OPCAB survival rates are calculated to be 89.4% and many patients report great improvement from symptoms like chest discomfort (angina) and better heart function. Long-term results are positive, and for the right individuals, the treatment is regarded as a safe and efficient substitute for standard CABG. The decision to undergo OPCAB or conventional CABG, however, depends on several variables, including the patient’s general health, the intricacy of the CAD, and the surgeon’s experience. OPCAB is a helpful option for the management of CAD as it develops along with improvements in surgical methods and tools. (John Hopkins Medicine)
iii. Minimally Invasive Direct Coronary Artery Bypass (MIDCAB)
A cutting-edge surgical procedure called minimally invasive direct coronary artery bypass (MIDCAB) was developed to treat CAD with less invasiveness than conventional open-heart surgery. To access the heart during MIDCAB, a tiny incision is often made on the left side of the chest. MIDCAB is performed without a heart-lung bypass machine, in contrast to traditional CABG. Instead, the target coronary artery can be operated on while the heart is still beating due to the sophisticated equipment that stabilizes the heart. To access the blocked coronary artery, small thoracotomy incisions are performed. A graft, frequently taken from the internal mammary artery or radial artery (one of two continuations of the brachial artery. It supplies the anterior compartment of the forearm), is then directly sutured onto the artery to bypass the obstruction. For patients with adequate coronary anatomy and disease features, this approach offers a few benefits, including decreased surgical trauma, quicker recovery durations, and a potentially faster return to regular activities. For some patients with CAD, MIDCAB offers a less invasive approach, which is a significant improvement in cardiac surgery.
a. Percutaneous Coronary Inventions (PCI)
Modern cardiology’s cornerstone, percutaneous coronary intervention (PCI), is a minimally invasive interventional technique used to treat CAD. To access the damaged coronary artery section during PCI, a thin, flexible catheter outfitted with a balloon-tipped angioplasty catheter is inserted through the femoral or radial arteries. The atherosclerotic plaque (condition that develops when a sticky substance called plaque builds up inside your arteries) is then compressed against the artery wall by the balloon’s inflation at the site of the stenosis (narrowing), widening the clogged conduit. In many instances, a coronary stent is used to maintain artery patency following angioplasty, reducing the risk of restenosis. These stents are frequently drug-eluting. This method lessens ischemic heart symptoms, reduces angina, and improves myocardial perfusion. PCI requires careful patient selection based on coronary anatomy, lesion complexity, and clinical presentation even though the procedure is minimally invasive. Because it provides quick symptom alleviation and potentially life-saving therapies in acute coronary syndromes and scenarios including elective revascularization, it is an essential therapeutic modality in the toolbox for managing CAD (Cleveland Clinic, 2021).
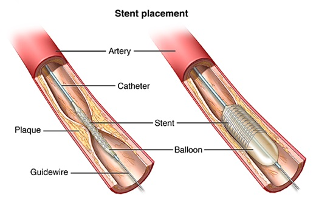
b. Angioplasty and Stent Placement
Crucial interventional techniques in the field of cardiology include angioplasty and stent placement, often known as percutaneous transluminal coronary angioplasty (PTCA) and coronary stent implantation. In this minimally invasive procedure, the damaged coronary artery segment is reached by navigating a flexible catheter fitted with a balloon angioplasty catheter through the femoral or radial artery. The atherosclerotic plaque (atheroma) is gently squeezed against the artery intima during the “dilatatio” process, which involves inflating the balloon at the location of the stenosis. This procedure restores luminal patency. An expertly placed coronary stent, frequently drug-eluting, is used, a procedure known as “stentio,” to guarantee prolonged artery integrity and prevent restenosis. The coronary artery is scaffolded by the stent, which is commonly made of biocompatible metals like cobalt-chromium or stainless steel. This allows for continued blood flow while preventing the development of neointimal hyperplasia. In contrast to conventional CABG, this method offers a less invasive option with a speedy patient recovery. The care of CAD has been revolutionized by PCI, which includes angioplasty and stent implantation. PCI is now a crucial therapeutic option in modern cardiology (NHS, 2022).

iv. Hybrid Approaches; Bypass and Angioplasty
A sophisticated therapeutic strategy for treating complicated CAD is hybrid coronary revascularization, which involves the concurrent use of surgical bypass and angioplasty procedures. The precision of conventional CABG is combined with the least invasive features of PCI in this hybrid method. A surgical cardiovascular expert performs a minimally invasive coronary artery bypass during this complex treatment to treat particular high-risk coronary lesions, frequently using internal mammary artery grafts. An interventional cardiologist performs angioplasty simultaneously using catheter-based procedures, which involves balloon dilatation of stenotic coronary arteries followed by the placement of drug-eluting stents. By balancing the minimally invasiveness of angioplasty with the durability of surgical grafts, this dual modality technique provides a customized approach for treating CAD. In preparing and carrying out these complex hybrid procedures, collaboration between cardiac surgeons and interventional cardiologists is essential for optimizing patient outcomes in cases of complex coronary artery disease (Annals of Thoracic Surgery, 2019).
v. Emerging Technologies and Procedures
Cardiology’s cutting-edge techniques and technologies constitute a vibrant new frontier in the never-ending quest for better patient care and results. New methods and technology are constantly changing the field of cardiac treatments as science and innovation progress. These innovations cover a variety of treatments, including minimally invasive mitral valve repair methods, percutaneous left ventricular assist devices (LVADs), and transcatheter aortic valve replacement (TAVR) for aortic valve dysfunction. Additionally, machine learning and AI are being used in predictive analytics to help identify individuals, who are at high risk for cardiac events. These new frontiers are pushing the limits of what is possible in the treatment of cardiovascular diseases, and they offer patients with heart ailments a better future with more efficient, less invasive, and individualized care.
a. Transmyocardial Laser Revascularization (TMR)
When traditional treatments fail to control CAD, transmyocardial revascularization (TMR) surgery represents a significant development in the therapeutic toolbox. TMR uses direct routes through the myocardium to bypass blocked coronary arteries and restore blood flow to ischemic parts of the heart. This ground-breaking method makes use of a specific laser system and frequently uses carbon dioxide (CO2) as an energy source. In order to reach the left ventricle during TMR, the patient is routinely given general anesthesia and has a left thoracotomy. A laser catheter is then cautiously inserted into the myocardium after that. A precise tunnel is subsequently made through the ventricular wall and into the ischemic tissue by the laser’s energy discharge. By using CO2 as the laser medium, nearby tissues are protected from heat damage. These channels promote neovascularization, or the growth of new blood vessels, which improves cardiac perfusion. TMR has a distinct advantage in treating complicated CAD cases and refractory angina because it does not require patent coronary arteries, potentially offering a last resort for patients with few curative options. This painstaking process highlights the importance of CAD management through the integration of surgical accuracy, laser technology, and creative thinking (Institute for Advanced Reconstruction, 2023).
b. Atherectomy
The exact removal of atherosclerotic plaque from coronary arteries is the goal of the specialist interventional treatment known as atherectomy, which is used in the management of CAD. This procedure is normally carried out in a catheterization lab. A dedicated atherectomy catheter is first inserted into the target coronary artery section during the surgery under the guidance of fluoroscopy and intravascular imaging techniques. Rotational atherectomy, directional atherectomy, orbital atherectomy, and laser atherectomy are only a few of the mechanical and laser-based procedures used in atherectomy, each of which is designed to target a different lesion characteristic. In terms of mechanics, atherectomy entails the mechanical abrasion, excision, or debulking of the plaque in order to improve blood flow and restore luminal patency. In laser atherectomy, the atherosclerotic plaque is vaporized and emulsified using a focused laser beam. Lesion morphology and operator skill are taken into consideration while choosing an atherectomy mode. When treating severely calcified or fibrous plaques, atherectomy has been found to be beneficial where balloon angioplasty or stent implantation alone may not be. This intervention is a crucial part of current CAD care since it offers a focused strategy for removing plaque, which improves coronary blood flow and improves patient outcomes.
c. AI-assisted Surgeries
AI is a revolutionary force that has reshaped technology in a variety of fields in the modern era. Particularly in the context of CAD procedures, the discipline of cardiology has seen dramatic improvements spurred by AI. The seamless integration of powerful AI algorithms with surgical robotic systems has made AI-assisted surgeries a potential new field, greatly improving both decision-making and precision. With a revised approach to CAD treatment, this synergistic combination of human experience and computational intelligence shows great promise for lowering mortality rates and speeding up patient recovery. The preoperative planning stage of AI’s involvement involves analysis of patient-specific data, including medical history, diagnostic testing, and imaging, to produce individualized treatment plans that optimize graft selection and procedural techniques. AI enables real-time intraoperative decision support during the surgical procedure itself, improving surgical precision and reducing human error. Modern AI-driven robotic systems integrate cutting-edge imaging technologies and provide steady instrument control, allowing surgeons to see the morphology of the coronary arteries, the inside of the plaques, and the dynamics of blood flow. AI analyzes this data and gives surgeons immediate feedback to help them perform precise stent placement and graft anastomosis. These improvements in procedural precision could lessen complications and thus cut fatality rates. AI is also used in postoperative care, where machine learning algorithms continuously monitor patients’ vital signs, lab findings, and imaging data in order to quickly spot any indicators of difficulties. This capability for early intervention may lessen the severity of probable post-surgical problems, thereby speeding up recovery. Predictive analytics powered by AI are also essential for optimizing prescription schedules and determining long-term prognosis, enabling personalized medicine, evidence-based therapy. While the full effects of AI-assisted CAD procedures are still being studied, preliminary results point to the possibility of better surgical results, fewer problems, and faster patient recovery. The integration of AI into surgical practice suggests a future in which technological prowess and medical expertise converge to redefine the standard of care in the field of CAD treatment, possibly changing the statistics of patient mortality and recovery times in cardiovascular surgery (NHS, 2023).
8. Conclusion
In summary, AI has been hugely developed in the field of CAD over the past few years. The precision that AI has to offer is remarkable and has shown huge potential in improving clinical performance. From clinical decision support systems to highly accurate cardiovascular disease prediction, AI brings a whole new area of innovation to cardiology. The use of AI in cardiovascular science and care is bound to bring endless ground-breaking successes. In this review paper, it was discussed how AI can assist in the risk stratification, diagnosis, and surgery of CAD. However, it is important to note that there is still much to discover and develop before AI can be implemented in everyday clinical practices. All in all, AI has proved itself a driving force in the future of medicine and is here to stay.
References
Acharya, U. R. Fujita, H. Lih, O. S. Adam, M. Tan, J. H. Chua, C. K. (2017) ‘Automated detection of coronary artery disease using different durations of ECG segments with convolutional neural network.’ Knowledge-Based Systems, 132, 62–71. Available at: https://linkinghub.elsevier.com/retrieve/pii/S0950705117302769 (January 18th 2023)
Acharya, U. R., Hagiwara, Y., Koh, J. E. W., Oh, S. L., Tan, J. H., Adam, M., & Tan, R. S. (2018) ‘Entropies for automated detection of coronary artery disease using ECG signals: A review.’ Biocybernetics and Biomedical Engineering, 38 (2), 373-384. Available at: https://www.sciencedirect.com/science/article/abs/pii/S0208521618300032 (January 18th 2023)
ACURATE neo2TM Aortic Valve System (no date). Available at: https://www.bostonscientific.com/en-EU/medical-specialties/structural-heart/tavi-acurate-neo2.html?utm_source=google&utm_medium=search-brand_paid&utm_campaign=ic-sh-emea_en-acurateneo2_paid_search-hcp&utm_content=main_5-search-n-n&cid=ps10012944&gclid=Cj0KCQjwuZGnBhD1ARIsACxbAVhmc3tgRTOcQ179Ctv5qP6nP0GOdIkwD8NvD6lf1qm39ljJkLSCcxoaAkL9EALw_wcB.
AI is poised to “Revolutionize” surgery (no date). Available at: https://www.facs.org/for-medical-professionals/news-publications/news-and-articles/bulletin/2023/june-2023-volume-108-issue-6/ai-is-poised-to-revolutionize-surgery/.
American Lung Association (no date) Thoracotomy. Available at: https://www.lung.org/lung-health-diseases/lung-procedures-and-tests/thoracotomy#:~:text=A%20thoracotomy%20is%20a%20surgical,be%20used%2C%20but%20is%20rare.
Bachar, B.J. (2023). Coronary artery bypass graft. Available at: https://www.ncbi.nlm.nih.gov/books/NBK507836/.
BBC News. (2010). Private clinic proves cheaper for NHS patients. Available at: https://www.bbc.co.uk/news/health-10789246 (Accessed: 19th August 2023).
Bodenstedt, S. et al. (2020) “Artificial Intelligence-Assisted Surgery: Potential and challenges,” Visceral Medicine, 36(6), pp. 450–455. Available at: https://doi.org/10.1159/000511351.
Brown, JC. Gerhardt, TE. Kwon E. (2023) ‘Risk Factors for Coronary Artery Disease’, StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK554410/ (January 18th 2023)
Cardiovascular Business (2023) Cardiology has embraced AI more than most other specialities. Available at: https://cardiovascularbusiness.com/topics/artificial-intelligence/cardiology-has-embraced-ai-more-most-other-specialties (Accessed: 22nd August 2023).
Centers For Disease Control and Prevention (2021) Coronary Artery Disease (CAD). Available at: https://www.cdc.gov/heartdisease/coronary_ad.htm (Accessed 18 August 2023)
Cheesborough, J.E. et al. (2015) “Targeted muscle reinnervation and advanced prosthetic arms,” Seminars in Plastic Surgery, 29(01), pp. 062–072. Available at: https://doi.org/10.1055/s-0035-1544166.
Cleveland Clinic (2023) Coronary Artery Disease. Available at: https://my.clevelandclinic.org/health/diseases/16898-coronary-artery-disease (Accessed 18 August 2023)
Coronary artery bypass graft (2023). Available at: https://pubmed.ncbi.nlm.nih.gov/29939613/.
Coronary artery bypass graft Surgery (2021). Available at: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/coronary-artery-bypass-graft-surgery.
Daiber A, and Münzel T. (2015). Organic Nitrate Therapy, Nitrate Tolerance, and Nitrate-Induced Endothelial Dysfunction: Emphasis on Redox Biology and Oxidative Stress. Antioxid Redox Signal. 23(11):899-942. [PMC free article] [PubMed]
Edureka! (2023) Types Of Artificial Intelligence You Should Know Available at: https://www.edureka.co/blog/types-of-artificial-intelligence/#Branches%20Of%20Artificial%20Intelligence (Accessed August 22 2023)
Edureka! (2023) What is Deep Learning? Getting Started With Deep Learning Available at: https://www.edureka.co/blog/what-is-deep-learning (Accessed Aug 22, 2023)
Gonzalez, A. (2021) What is an atherectomy? Available at: https://www.webmd.com/heart-disease/what-is-atherectomy.
Gücük, A. Üyetürk, U. (2014) ‘Usefulness of Hounsfield unit and density in the assessment and treatment of urinary stones’, World Journal of Nephrology, 3 (4), 282-286. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4220362/ (January 18th 2023)
Hayıroğlu, M.İ. and Altay, S. (2023). “The role of artificial intelligence in coronary artery disease and atrial fibrillation,” Balkan Medical Journal, 40(3), pp. 151–152. Available at: https://doi.org/10.4274/balkanmedj.galenos.2023.06042023.
Head, S.J. et al. (2013). “Coronary artery bypass grafting: Part 1–the evolution over the first 50 years,” European Heart Journal, 34(37), pp. 2862–2872. Available at: https://doi.org/10.1093/eurheartj/eht330.
Head, S.J. et al. (2013). “Coronary artery bypass grafting: Part 1–the evolution over the first 50 years,” European Heart Journal, 34(37), pp. 2862–2872. Available at: https://doi.org/10.1093/eurheartj/eht330.
Healthline (2023). Long-Term Blood Thinner Use: What You Need To Know. Available at: https://www.healthline.com/health/living-with-atrial-fibrillation/advancements/long-term-blood-thinner-use#how-blood-thinners-work (Accessed: 19th august 2023).
Healthline. (2018). The History of Heart Disease. Available at: https://www.healthline.com/health/heart-disease/history#the-future-of-heart-disease (Accessed: 19th August 2023).
Heart Foundation, Coronary Artery Calcium Scoring. Available at: https://www.heartfoundation.org.au/bundles/your-heart/medical-tests-coronary-artery-calcium-score#:~:text=A%20coronary%20artery%20calcium%20score%20is%20a%20measure%20of%20how,nutrients%20that%20reach%20your%20heart (January 18th 2023)
Heron M, Anderson RN. (2016). Changes in the leading cause of death: Recent patterns in heart disease and cancer mortality. NCHS Data Brief, no 254. Hyattsville, MD: National Center for Health Statistics.
Hogan, L. (2021). What to know about surgery for Coronary Artery Disease (CAD). Available at: https://www.webmd.com/heart-disease/what-to-know-surgery-coronary-artery-disease.
Hogan, L. (2021). What to know about surgery for Coronary Artery Disease (CAD). Available at: https://www.webmd.com/heart-disease/what-to-know-surgery-coronary-artery-disease.
Hogan, L. (2021b) What to know about surgery for Coronary Artery Disease (CAD). Available at:https://www.webmd.com/heart-disease/what-to-know-surgery-coronary-artery-disease.
Honeill. (2023). “What is Targeted Muscle Reinnervation (TMR) Surgery?,” The Institute for Advanced Reconstruction, 23 May. Available at: https://www.advancedreconstruction.com/blog/what-is-targeted-muscle-reinnervation-surgery.
Hopkins Medicine, Coronary Computed Tomography Angiography (CCTA). Available at: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/coronary-computed-tomography-angiography-ccta (January 18th 2023)
https://newsroom.osfhealthcare.org/heart-disease-rate-on-the-rise/ (January 18th 2023)
IBM (2023) What is deep learning? Available at: https://www.ibm.com/topics/deep-learning (Accessed Aug 22, 2023)
IBM (2023) What is machine learning? Available at: https://www.ibm.com/topics/machine-learning (Accessed August 22 2023)
International Business Machines, What are Convolutional Neural Networks? Available at: https://www.ibm.com/topics/convolutional-neural-networks (January 18th 2023)
Kang, D. Dey, D. Slomka, P. Arsanjani, R. Nakazato, R. Ko, H. Berman, D. Li, D. Kuo, J. (2015) ‘Structured learning Algorithm for detection of nonobstructive and obstructive coronary plaque lesions from computed tomography angiography’, Journal of Medical Imaging, 2 (1). Available at: https://doi.org/10.1117/1.JMI.2.1.014003 (January 18th 2023)
Kayatta, M.O., Halkos, M.E. and Narayan, P. (2018). “Minimally invasive coronary artery bypass grafting,” Indian Journal of Thoracic and Cardiovascular Surgery [Preprint]. Available at: https://doi.org/10.1007/s12055-017-0631-x.
Kayatta, M.O., Halkos, M.E. and Narayan, P. (2018b) “Minimally invasive coronary artery bypass grafting,” Indian Journal of Thoracic and Cardiovascular Surgery [Preprint]. Available at: https://doi.org/10.1007/s12055-017-0631-x.
Kayatta, M.O., Halkos, M.E. and Narayan, P. (2018c) “Minimally invasive coronary artery bypass grafting,” Indian Journal of Thoracic and Cardiovascular Surgery [Preprint]. Available at: https://doi.org/10.1007/s12055-017-0631-x.
Lessmann, N. van Ginneken, B. Zreik, M. de Jong, P. A. de Vos, B. D. Viergever, M. A., Isgum, I. (2018) ‘Automatic Calcium Scoring in Low-Dose Chest CT Using Deep Neural Networks With Dilated Convolutions’, IEEE Transactions on Medical Imaging, 37 (2), 615-625. Available at: https://ieeexplore.ieee.org/document/8094970 (January 18th 2023)
Lin, A. Kolossváry M. Motwani, M. Išgum, I. Maurovich-Horat, P. Slomka, P. Dey, D. (2021) ‘Artificial Intelligence in Cardiovascular Imaging for Risk Stratification in Coronary Artery Disease’, Radiological Society of North America, 3 (1). Available at: https://pubs.rsna.org/doi/epdf/10.1148/ryct.2021200512 (January 18th 2023)
MacGill, M. (2018) What should I expect during open heart surgery? Available at: https://www.medicalnewstoday.com/articles/312888#recovery.
MacGill, M. (2018b). What should I expect during open heart surgery? Available at: https://www.medicalnewstoday.com/articles/312888#:~:text=There%20is%20insufficient%20evidence%20to,at%20about%2096%E2%80%9397%20percent.
Madani, A. Arnaout, R. Mofrad, M. (2018) ‘Fast and accurate view classification of echocardiograms using deep learning’, npj Digital Medicine, 1 (6), Available at: https://doi.org/10.1038/s41746-017-0013-1 (January 18th 2023)
Maleki, M. Esmaeilzadeh, M. (2012) ‘ The evolutionary development of echocardiography’, Iran J Med Sci, 37 (4), 222-232. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3565194/#:~:text=%E2%80%9CThe%20origins%20of%20echocardiography%20date,discovery%20of%20piezoelectricity%20in%201880%E2%80%9D.&text=Ultrasound%20waves%20are%20created%20by,Helmuth%20Hertz%20and%20Inge%20Edler. (January 18th 2023)
Medical News Today (2022) What does an EKG for Coronary Artery Disease show? Available at: https://www.medicalnewstoday.com/articles/coronary-artery-disease-ecg (January 18th 2023)
Medtronic (no date b) Coronary Artery Disease – treatment Options | Medtronic. Available at: https://www.medtronic.com/us-en/patients/treatments-therapies/heart-surgery-cad/treatment-options.html.
Medtronic (no date c) Coronary Artery Disease – treatment Options | Medtronic. Available at: https://www.medtronic.com/us-en/patients/treatments-therapies/heart-surgery-cad/treatment-options.html.
Medtronic (no date) Coronary Artery Disease – treatment Options | Medtronic. Available at: https://www.medtronic.com/us-en/patients/treatments-therapies/heart-surgery-cad/treatment-options.html.
National Library of Medicine (2019) Overview of artificial intelligence in medicine. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6691444/ (Accessed 19 August 2023)
National Library of Medicine. (2021). Artificial intelligence and cardiac surgery during COVID-19 era. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8013221/#:~:text=The%20operative%20mortality%20in%20patients,0.80)%20using%20the%20logistic%20EuroSCORE. ( Accessed:19th August 2023).Artificial intelligence and cardiac surgery during COVID‐19 era – PMC
National Library of Medicine. (2023). Nitrates. Available at: https://www.ncbi.nlm.nih.gov/books/NBK545149/ (Accessed: 22nd August 2023).
Ngu, J.M.C., Sun, L.Y. and Ruel, M. (2018). “Pivotal contemporary trials of percutaneous coronary intervention vs. coronary artery bypass grafting: a surgical perspective,” Annals of Cardiothoracic Surgery, 7(4), pp. 527–532. Available at: https://doi.org/10.21037/acs.2018.05.12.
NHS. ( 2022). Cardiac catheterisation and coronary angiography. Available at: https://www.nhs.uk/conditions/coronary-angiography/#:~:text=What%20happens%20during%20coronary%20angiography,the%20heart%20and%20coronary%20arteries (Accessed:19th August 2023).
NHS. (2020). Treatment Coronary heart disease. Available at: https://www.nhs.uk/conditions/coronary-heart-disease/treatment/ (Accessed: 19th August 2023).
NHS. (2023) Treatment. Available at: https://www.nhs.uk/conditions/coronary-heart-disease/treatment/.
NHS. (2023a). Angina. Available at: https://www.nhs.uk/conditions/angina/#:~:text=Angina%20is%20chest%20pain%20caused,of%20these%20more%20serious%20problems.
NHS. (2023b) Coronary artery bypass graft. Available at: https://www.nhs.uk/conditions/coronary-artery-bypass-graft-cabg/.
NHS. (2023d). Coronary artery bypass graft. Available at: https://www.nhs.uk/conditions/coronary-artery-bypass-graft-cabg/#:~:text=A%20coronary%20artery%20bypass%20graft,oxygen%20supply%20to%20the%20heart.
NHS. (2023e) Treatment. Available at: https://www.nhs.uk/conditions/coronary-heart-disease/treatment/.
NHS. (2023f) Treatment. Available at: https://www.nhs.uk/conditions/coronary-heart-disease/treatment/.
Off-Pump coronary artery bypass surgery. (2019). Available at: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/offpump-coronary-artery-bypass-surgery.
OSF Healthcare (2022) Heart Disease Rate on the Rise. Available at:
Powerful Medical (2023) How is AI transforming ECG interpretation? Available at: https://www.powerfulmedical.com/blog/how-is-ai-transforming-ecg-interpretation (January 18th 2023)
Professional, C.C.M. (no date). Percutaneous coronary intervention. Available at: https://my.clevelandclinic.org/health/treatments/22066-percutaneous-coronary-intervention.
Sef, D. and Raja, S.G. (2021) “Bilateral internal thoracic artery use in coronary artery bypass grafting in the post-ART era – Perspective,” International Journal of Surgery, 86, pp. 1–4. Available at: https://doi.org/10.1016/j.ijsu.2020.12.007.
Semenza, G.L. (2000) “Series Introduction: Tissue ischemia: pathophysiology and therapeutics,” Journal of Clinical Investigation, 106(5), pp. 613–614. Available at: https://doi.org/10.1172/jci10913.
Surgery for coronary artery disease (no date b). Available at: https://nyulangone.org/conditions/coronary-artery-disease/treatments/surgery-for-coronary-artery-disease.
Surgery for coronary artery disease (no date). Available at https://nyulangone.org/conditions/coronary-artery-disease/treatments/surgery-for-coronary-arterisease.
Surgery for coronary artery disease (no date). Available at: https://nyulangone.org/conditions/coronary-artery-disease/treatments/surgery-for-coronary-artery-disease.
Surgical Procedures for Coronary artery Disease | Cardiac Surgery | SUNY Upstate Medical University (no date). Available at: https://www.upstate.edu/cardiacsurgery/surgical-procedures/cad-procedures.php
Targeted Muscle Reinnervation | Tampa General Hospital (no date). Available at: https://www.tgh.org/institutes-and-services/treatments/targeted-muscle-reinnervation-tmr.
Traditional heart surgery (no date). Available at: https://www.cedars-sinai.org/programs/heart/clinical/cardiac-surgery/traditional.html.
Website, N. (2022). Coronary angioplasty and stent insertion. Available at: https://www.nhs.uk/conditions/coronary-angioplasty/.
What To Expect During Targeted Muscle Reinnervation Surgery (2023). Available at: https://healthcare.utah.edu/plastic-surgery/reconstructive/targeted-muscle-reinnervation-tmr.
Yamashita, K. et al. (2017). “Long-term outcome of isolated off-pump coronary artery by pass grafting in patients with coronary artery disease and mild to moderate aortic stenosis,” Journal of Cardiology [Preprint]. Available at: https://doi.org/10.1016/j.jjcc.2016.10.007.
Yip, M.C. et al. (2023) “Artificial intelligence meets medical robotics,” Science, 381(6654), pp. 141–146. Available at: https://doi.org/10.1126/science.adj3312.
Yu, C. (2017) ‘Challenges and opportunity in the era of quantitative echocardiography’, Echo Res Pract, 4 (4), E3-E6. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5633054/ (January 18th 2023)




{kind=link}