
Table of Contents
Section I: Neurodevelopmental Impacts of Bullying
Amayel Camara, Reine Khoury, Dimitri Krontiras, SolBean Lee, Elsa Macpherson, Fatima Raza, Sarah Shareef
– 1. Introduction
– 2. In-Person Bullying
– – 2.1 Psychological Aspects
– – 2.2 Neurological Aspects
– 3. Cyberbullying
– – 3.1 Psychological Aspects
– – 3.2 Neurological Aspects
– 4. Discussion and Conclusion
Section II: PTSD, Memory and Learning
Emma Antonazzo, Siwei Guo, Ravine Jackson, Dongyoon Kim, Bhuvika Kodali, Lucy Ma, Olivia Mudrak, Sayuri Yamashita
– 1. Introduction
– 2. How Do Chemical Messengers Contribute to Memory Dysfunction?
– – 2.1 Baseline Role of Chemical Messengers
– – 2.2 Dysregulation of Chemical Messenger Systems in PTSD Patients
– – 2.3 Learning in PTSD Patients
– 3. ADHD and PTSD: Different Roots of Episodic Memory Impairment
– – 3.1 ADHD and Episodic Memory Aspects
– – 3.2 PTSD and Episodic Memory Aspects
– – 3.3 Overlap and Misdiagnosis
– 4. Discussion and Conclusion
Section I: Neurodevelopmental Impacts of Bullying
Amayel Camara, Reine Khoury, Dimitri Krontiras, SolBean Lee, Elsa Macpherson, Fatima Raza, Sarah Shareef
1. Introduction
Bullying is the intentional and prolonged action of enacting harm upon another person; this can take multiple forms, such as physical abuse or verbal abuse, and can occur at multiple different instances, like in-person and/or online. At younger ages, bullying and harassment are prominent in educational environments, especially amongst peers (Juvonen, Wang & Espinoza, 2010), with approximately one in three students being subject to multiple forms of abuse (Mbah, 2020). Consequences of bullying can develop over time and have a negative impact on one’s wellbeing that continues into adulthood, including persistent feelings of insecurity, loneliness and isolation. While several cognitive processes can be affected, physical consequences can arise from bullying too; these can include sleep disturbances, headaches and more (Rivara et al., 2016). This is a particular concern among children and adolescents, as this crucial period of biological and psychological development is most vulnerable to stressors such as bullying (Connaughton et al., 2024).
One thing that these consequences have in common is that they may be a result of changes within the neurobiological aspects of the brain (Bates, 2015). Palamarchuk and Vaillancourt (2022) state that “psychological stress is a physiological response to a salient stimulus that is perceived as a stressor [] and thus triggers neurocognitive reactivity to adapt”. Through MRI findings, it is suggested that childhood bullying can result in alterations in the brain structure due to “stress-induced neuroendocrine reactivity, neuromodulation and limbic system dysregulation”. The brain’s attempts to manage persistent stress of bullying have been further linked to the overactivation of the limbic system, particularly the amygdala and hippocampus, potentially resulting in increased volume in these regions” (Palamarchuk & Vaillancourt, 2022). For this reason, it is widely believed that childhood bullying has widespread effects on brain development due to “a complex mix of adaptive and degenerative effects”.
However, the studies above fail to take into consideration the nuances of various bullying styles; this distinction is important, as in-person bullying often involves immediate physical or verbal threats, while cyberbullying’s 24/7 nature and public permanence may exacerbate feelings of helplessness (Smith et al., 2023). To better capture the complexity, the analysed consequences of bullying should not be excessively generalised to understand the influences of various bullying styles accurately. Therefore, Section I of our paper observes the effects of in-person and cyberbullying, addressing physical aspects through the analysis of research on in-person bullying and verbal aspects through the analysis of research on cyberbullying. This helps narrow down the inaccuracies within subgroups and can aid in creating prevention plans for specific subdivisions.
2. In-Person Bullying
Traditionally, bullying among adolescents takes place in person and is often a direct form of both verbal and physical abuse; peer bullying commonly happens within an educational environment, leading victims to feel trapped due to forced proximity. Between April 2022 and March 2023, the Office for National Statistics found that an estimated 34.9% of children aged 10-15 experienced in-person bullying in the UK (ONS, 2021).
In-person bullying may also involve physical violence during confrontations; experiencing violence at the hands of peers during the developmental stages may lead to short-term physical repercussions on the child’s health. These responses, in some cases, can also cause a lingering effect on the body and the mind throughout adulthood. The biological effects of violence have become increasingly better understood, including the effects on the brain, neuroendocrine system and immune response. Consequences may include increased incidences of depression, anxiety, post-traumatic stress disorder (PTSD), suicide, increased risk of cardiovascular disease and premature mortality (Rivara et al., 2019).
Additionally, researchers found strong associations between the perpetrators of bullying and those who experience interparental violence, living with non-biological parents and high strengths and difficulties questionnaire scores. This suggests that perpetrators of childhood bullying often undergo adverse childhood experiences, and therefore, peer abuse is often a reflection of trauma caused by external abuse that a child might experience. Maltreatment between young peers is a complex issue which we will further explore within this article by analysing both the psychological and neurobiological effects bullying within adolescence can have on a child’s development.
2.1 Psychological Aspects
In-person bullying from a psychological standpoint shows the enervating and crippling harm it does to individuals. Such victims at a young age are seen to suffer the immediate psychological effects right after the point of the incident, having to endure the longitudinal consequences during adulthood. The immediate symptoms after a traumatic event has occurred can lead to children developing anxiety and hypervigilance when they are in social situations; they are also seen to develop the idea that they are helpless and that there is minimal assistance at their disposal (Mulenga, Kakupa & Xia, 2025). In addition, there can be a decrease in self-worth and self-esteem, which explains how these individuals can have a gradual decline in academic success (Zhao et al., 2024; Rivara et al., 2019).
The relentless effects of in-person bullying have been seen to simultaneously present longitudinal consequences upon their respective victims; they may exhibit external issues, along with hiding their internal issues from others. Internalised issues may include depression, anxiety and fear (Renzo Abregú-Crespo et al., 2023). External issues may include anger and aggression towards others; conduct disorder, substance abuse issues and impulsive behaviour can also be accounted for as additional factors (Renzo Abregú-Crespo et al., 2023). As some victims may become more aggressive, they may turn into bullies themselves. According to Bandura (1963), Social Learning Theory explains how children learn by observing the behaviours they have witnessed. If they have observed behaviour that is aggressive, they could shape their behaviour to match in order to communicate their frustrations.
2.2 Neurological Aspects
In-person bullying from a neurological standpoint reveals significant and long-term alterations in the brain. Victims at young ages can display both immediate and long-term neurological shifts. For instance, bullying has been shown to dysregulate the hypothalamic-pituitary-adrenal (HPA) axis, producing abnormal cortisol responses to stress. Sometimes they can be elevated or depleted, depending on the context, but still ultimately impair emotional regulation and stress adaptation (Chen et al., 2025; Vaillancourt, 2018). Moreover, cortisol dysregulation during this stage of adolescence can be linked to a plethora of factors, both internal and external, potentially affecting academic and social outcomes (Du Plessis et al., 2019).
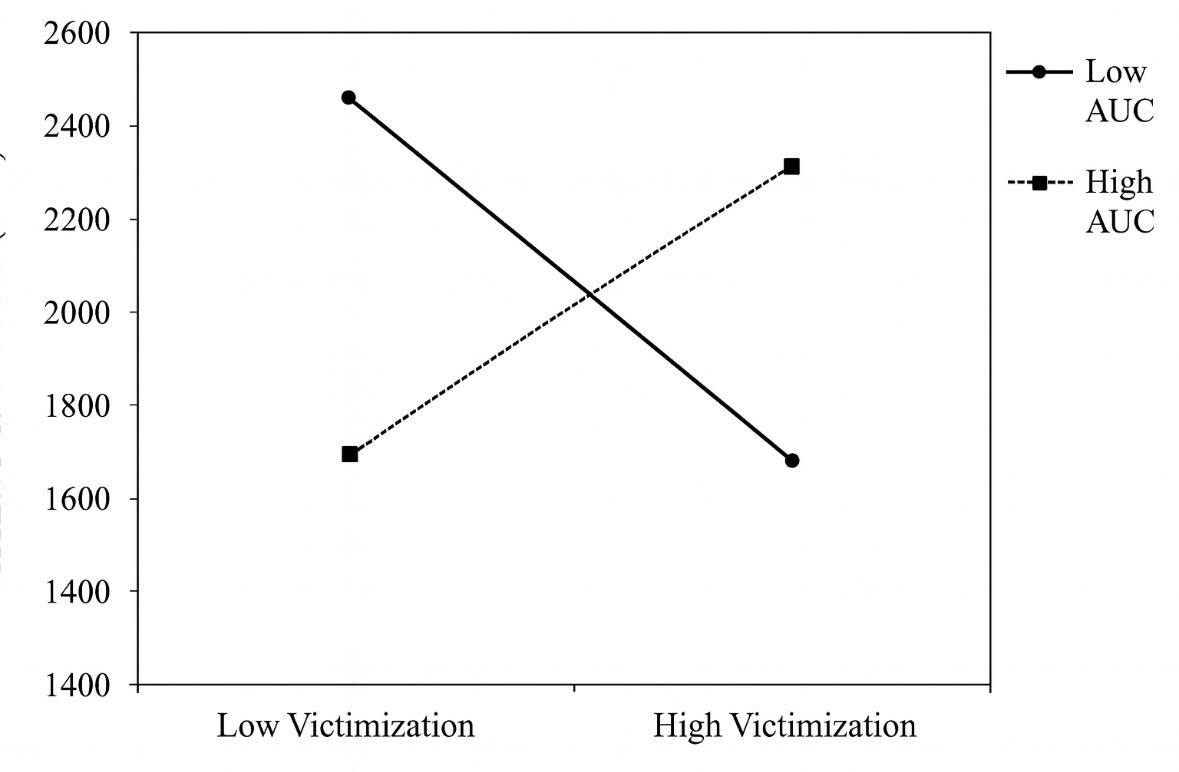
Neuroimaging studies show that bullying alters structural and functional brain development. One study found that boys with different cortisol levels exhibited changes in the ventrolateral prefrontal cortex (vlPFC) structure in response to peer victimisation; it was seen that cortisol output was significantly associated with a small vlPFC surface area, while high cortisol output was associated with larger areas (Du Plessis et al., 2019). Additionally, MRI scans showed thickening in the cortex in the fusiform gyrus in bullied children, which suggests that their developmental trajectories were significantly altered in regions involved in face processing (Palamarchuk et al., 2022).
Figure 1: Peer victimisation levels and prefrontal cortex development (Du Plessis et al., 2019).
Figure 2: Cortical thickness differences in bullied children (Palamarchuk et al., 2022).
Functionally, bullied adolescents show heightened amygdala, ventral striatum, medial prefrontal cortex and insula activation when exposed to social stimuli, pointing to changes in socioemotional processing networks (Perino et al., 2019). Broader work on stress effects indicates that connectivity between the prefrontal cortex and hippocampus/amygdala (the parts of the brain in charge of emotional regulation) is weakened by stress. This mechanism can foreshadow persistent negative memories of bullying leading up to adulthood (Rivara et al., 2016; Vaillancourt et al., 2011).
Taken together, these findings underscore that bullying not only affects the brain on a psychological standpoint, but can ultimately alter stress responses and typical cortisol levels, dysregulating emotional processing pathways, often with persistent effects into adolescence and beyond.
3. Cyberbullying
Cyberbullying is more than just “online teasing”; it is the intentional act of harming others repetitively using digital technologies. Prevalence estimates suggest that 30–45% of adolescents worldwide experience online victimisation (Pew Research Center, 2022). Therefore, cyberbullying has become a worldwide problem affecting both physiological and neurological aspects.
Unlike in-person bullying, which happens at physical locations, cyberbullying has no specific limitations, since it can take place at any time and from any location. This form of hostile behaviour lacks personal contact, which is its hallmark, along with anonymity, broad scope and the capacity to inflict long-lasting damage. Typical examples of cyberbullying include cyberstalking, masquerading, cyber exclusion and flaming, which may occur simultaneously or at different times and are further compounded by the internet (Tokunaga, 2010; Partington et al., 2020). There are many given reasons which may differ from one user to another to explain the phenomenon of cyberbullying, such as the wish to attain a certain level of social esteem, revenge of some kind, entertainment and even pressure from peers (Ding, Lin & Chen, 2025). Cyberbullying can affect mental wellbeing, social connections and behaviour. Its 24/7, permanent and public nature often makes its effects more intense than in-person bullying. Studies have found that victims of cyberbullying were 2.3 times more likely to experience depressive symptoms than those not exposed (John et al., 2018).
It was found that 57% of students had experienced cyberbullying at least once or twice through different types of media (Peled, 2019). Furthermore, mental health systemic reviews reveal consistent links to academic underachievement, poor school attendance, victimisation and interpersonal difficulties (Chen et al., 2025). One considerable case is Discord, a platform initially created for gaming communities, now a social network, which illustrates some of the difficulties in addressing cyberbullying. Statistics indicate that harassment and bullying make up nearly 19% of all user-submitted behaviour on Discord, and approximately 7% of reported cyberbullying incidents among youth occur on this platform (Statista, 2023). Discord is a prime example of modern cyberbullying, illustrating how platform design can influence both the prevalence and intensity of online harassment.
3.1 Psychological Aspects
The psychological consequences of cyberbullying are often severe and debilitating, extending beyond simple, temporary sadness. The persistent nature of the harassment means that there is limited safety, especially due to the lack of online privacy, eventually leading to a state of hypervigilance and chronic stress as victims anticipate cyberbullying attacks at any hour (Wilson & Sun, 1984; Tokunaga, 2010). This aligns with the broader evidence that cyberbullying, with its constant accessibility, unavoidability and lasting digital records, often intensifies psychological damage beyond that of traditional bullying (Kowalski et al., 2014). The permanent nature of online content facilitates re-victimisation, as harmful posts or messages can be revisited, screenshotted and shared indefinitely, preventing emotional wounds from healing and reinforcing feelings of powerlessness for the victim. This toxic cycle can manifest in clinically significant symptoms, including social withdrawal, sleep disturbances, somatic complaints like headaches and stomachaches, and a loss of interest in activities once enjoyed (Kowalski et al., 2014; Gini & Pozzoli, 2013).
Studies highlight that cyberbullying involvement (reported by 14.17% of participants) is significantly linked to lower self-esteem and higher anxiety and depression (Mbah, 2020). The fear of public judgement, and of humiliation, systematically erodes self-worth, creating feelings of isolation and shame (Wetherall, Robb & O’Connor, 2019). For some, like with in-person bullying, this overwhelming distress can trigger suicidal ideation and self-harming behaviours, representing the most tragic outcome of this digital abuse (Van Geel, Vedder & Tanilon, 2014). These negative effects are not ephemeral as they often persist into adulthood, shaping long-term life trajectories by influencing self-perception, the ability to trust others and overall mental well-being (Shah et al., 2022).
Furthermore, the risks of undergoing cyberbullying are not distributed equally: adolescents with pre-existing mental health conditions or marginalised identities with limited peer support face compounded risks (Shah et al., 2022). For these more vulnerable teenagers, cyberbullying is not an isolated stressor but a dangerous multiplier of pre-existing psychological distress, potentially impeding recovery and access to care. The cumulative impact also creates a negative feedback loop, where the associated anxiety and depression disrupt academic focus, causing school failure, which further diminishes self-esteem and hope for the future (Juvonen & Graham, 2014).
3.2 Neurological Aspects
In addition to the psychological consequences of cyberbullying, neurological impacts have also been observed via functional MRI (fMRI), electroencephalogram (EEG) and the analysis of the cortisol secretion profile (McLoughlin et al., 2019; Prince et al., 2025; Ke et al., 2022; McLoughlin et al., 2022; González-Cabrera et al., 2017).
The most popular and perhaps ideal method is the usage of fMRI: a noninvasive imaging modality that provides an indirect measurement of brain activation by quantification of the haemodynamic response to a certain stimulus (McLoughlin et al., 2019). This allows researchers to analyse various brain regions and how they react to different conditions and stimuli. One example recognising this is research conducted by McLoughlin and her colleagues, which gathered a sample of 32 participants aged 18-25 to analyse the contrast between those who have been both cyberbullies and victims, only a cybervictim and neither. During the scan, participants observed a total of 12 scenarios resembling common social media posts with either a marginalised or positive comment. Results showed that, regardless of prior experience with cyberbullying, the L- and R- middle temporal gyrus (MTG) regions, as well as the L- and R- posterior cerebellum/vermis clusters, were activated in response to cyberbullying stimuli. This suggests that the participants were engaged in their social actions and emotions, while the posterior cerebellum can be linked to processing happiness and disgust (Zahn et al., 2007; Scheinle & Scharmüller, 2013). Alternatively, results indicated that those with no prior experience of cyberbullying showed a greater blood‐oxygenation‐level‐dependent (BOLD) response to the cyberbullying stimuli compared to the neutral stimuli in the L‐Precuneus, the area of the brain responsible for self‐evaluation and self‐consciousness. The researchers hypothesise that the participants imagined the scenario as a personal encounter (McLoughlin et al., 2019).
Furthermore, studies observing EEG results were used in Ke and her colleagues’ research to assess brain activity and functional connectivity associated with cyberbullying. They evaluated existing EEG stimuli on adolescents up to age 25 who had experienced cyberbullying, and came to the conclusion that there is, in fact, evidence for reorganisation within the reward system. The EEG evidence, measured by the grand-averaged reward‐related positivity (ReWP) event-related potential (ERP), indicated that the brain’s response to social acceptance was blunted. This suggests that peer-victimisation and cyberbullying, being social stressors, modified the activation within the reward network, which is responsible for processing and responding to rewarding stimuli (Ke et al., 2022). However, the article determined this method of observing neurological effects of peer victimisation as unreliable, as there was contradicting data shown by the EEG results and an increased brain activation in the amygdala (Ke et al., 2022). Overall, EEG is a method attempted to be utilised with minimal successful results.
As another approach towards investigating the neurological consequences of cyberbullying, González-Cabrera et al. (2017) observed the cortisol levels of saliva samples of 60 teenagers aged 12-18 labelled as cybervictims, cyberbullies, cyberbullied and victims, and cyberbystanders. Results showed that cortisol secretion was higher in cybervictims and cyberbully-victims than in other participants; the lowest cortisol secretion was shown in extreme cyberbullies, with a strong correlation between cyberbullying victimisation and the elevated profile of cortisol secretion. These cortisol production results, being stress hormones, indicate a correlation between cyberbullying victimisation and alterations in hypothalamic-pituitary-adrenal (HPA) axis function, which mediated an increase in stress of the participants.
4. Discussion and Conclusion
To summarise, while traditional, in-person forms of bullying can induce physical and mental forms of harm upon young individuals, cyberbullying seems to target the deep emotional systems of adolescents. Its peer-victimisation and unlimited accessibility allow it to inflict psychological distress that is often more severe and enduring than face-to-face aggression. The evidence consistently links cyberbullying to depression, poor academic performance and weakened social connections, showing its capacity to disrupt both personal development and educational outcomes. Thus, addressing cyberbullying requires a multifaceted approach that combines awareness, policy intervention and platform accountability to mitigate long-term consequences.
Cyberbullying leads to many adolescents feeling unsafe, as hateful comments and public humiliation can have severe longitudinal effects. Such persistent consequences can take away feelings of confidence, furthermore causing loneliness and anxiety. Cyberbullying or relentless stress can often lead to major struggles with controlling behaviours and emotions linked to both anxiety and self-worth.
Although there have been significant advancements in research regarding the neurobiological aspects of cyberbullying, there are still limitations to existing studies. For example, fMRI usage is modelled as pilot studies; therefore, they consist of smaller sample sizes and are unable to perform comparisons between genders as well as the contrast between cyberbully-victim, cybervictim and non-experienced individuals. Additionally, studies acknowledge the considerable overlap between bullying and cyberbullying, making it difficult to accurately analyse the impacts of only cyberbullying. Such adversity is also noted in the review analysing EEG results, which was unfortunately unable to distinguish the samples as it only considered cyberbullying and had to include all aspects of peer victimisation. Finally, the research on cortisol levels recognised that these results cannot apply to long-term effects, as they only analyse participants up to age 18. For now, until more studies are conducted in the future, these neurological results can only be recognised as impacts on adolescents.
The psychological and neurological consequences of in-person bullying demonstrate an idea for understanding how trauma can more broadly disrupt neurological processes like memory retention and cognition through PTSD. Psychologically, both bullying victims and individuals suffering from PTSD commonly exhibit heightened anxiety, paranoia and feelings of helplessness about their circumstances. Over time, these issues can develop into chronic internalised issues like depression and excessive fear, or become externalised through aggression and substance abuse. Neurologically, however, in-person bullying significantly alters the hypothalamic-pituitary-adrenal (HPA) axis and alters cortisol levels, causing a lack of stress axis regulation. This mirrors the cortisol-relation dysregulation that is linked to common symptoms of PTSD, such as memory dysfunction. Simultaneously, this highlights the changes in structures such as the prefrontal cortex, hippocampus and amygdala. Essentially, these findings have commonly suggested that both bullying and PTSD operate through a shared lens, reiterating how peer victimisation/bullying can affect and have long-lasting effects on cognition and mental health.
Overall, the results of studying traditional bullying and cyberbullying victimisation have long-term term impacts. Worldwide, bullying is a severe issue analysed among adolescents and children. If not taken seriously, these potential long-term consequences may continue into future generations. This review strongly encourages the development of a prevention and treatment plan in the future.
Section II: PTSD, Memory and Learning
Emma Antonazzo, Siwei Guo, Ravine Jackson, Dongyoon Kim, Bhuvika S. Kodali, Lucy Ma, Olivia Mudrak, Sayuri Yamashita
1. Introduction
In post-traumatic stress disorder (PTSD), the formation and encoding of episodic memories following a traumatic event profoundly impacts an individual’s mental state. It is a “chronic impairment disorder that occurs after exposure to traumatic events” (Miao et al., 2018). According to the DSM-5, diagnosis requires a stressor, intrusive symptoms (e.g., flashbacks and nightmares), avoidance of related stimuli, negative alterations in mood and cognition, and altered arousal and reactivity. Symptoms must last over a month, cause functional impairment in social or occupational situations and not be attributed to medication or substances. Intrusive flashbacks, a key symptom, are thought to be the result of undamped or persistent activation of pathological episodic memories (Brewin, 2014; Isaac et al., 2006; Moradi et al., 2008). An account of episodic memories consists of episodic elements, which are summary records of an experience, generally represented as visual images associated with a conceptual frame (Conway, 2009). This includes all the details of a specific memory, including the emotions felt during the time. In individuals with PTSD, an episodic memory can reactivate the emotions associated with the traumatic experience, resulting in a vivid re-living of the event, which negatively impacts their mental state.
The hormones cortisol and norepinephrine, contributing to the fight-or-flight response, are attributed to the encoding of these episodic memories. Levels are found to be significantly higher in individuals with PTSD, altering the efficiency of the neural pathways present throughout the limbic system, with predominant impact on the hippocampus (Tessner et al., 2007). The hippocampus, located deep within the temporal lobe and a part of the limbic system, plays a crucial role in the consolidation of information from short-term to long-term memory and is therefore essential to the encoding process of episodic memories.
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by impulsivity, hyperactivity and inattention (Sapkale & Sawal, 2023). There is a prevalent overlap between ADHD and PTSD symptoms, including emotional dysregulation, poor self-esteem and sleep irregularities, which leads to frequent misdiagnoses (Neff, 2021). Although episodic memories are dysfunctional in both disorders, the reasons differ: in PTSD, the disruption stems from trauma, whereas in ADHD, it is due to cognitive factors. In PTSD, episodic memory, regarding the traumatic event itself, is heightened with vivid emotional and sensory detail, partially due to overactivation of the amygdala (Pitts et al., 2022). However, neutral episodic memories of everyday life are impaired, resulting in vague memories (Pitts et al., 2022). On the other hand, ADHD episodic memory is fragmented due to impaired working memory, attention and recall difficulties, which are key characteristics of ADHD (Martin et al., 2023). Additionally, episodic memory is an essential foundation for learning as we use past experiences to absorb and retain new information. Therefore, when there are dysfunctions in episodic memory, as seen in PTSD and ADHD, educational challenges arise. To understand how these memories become so powerfully and pathologically encoded, we must first examine the chemical messengers that form the process.
2. How Do Chemical Messengers Contribute to Memory Dysfunction?
2.1 Baseline Role of Chemical Messengers
In a healthy brain, the encoding of episodic memories is a balanced chemical process, heavily reliant on two key messengers: norepinephrine (NE) and cortisol. Norepinephrine is a neurotransmitter important for attentiveness, emotions, sleeping, dreaming and learning. It functions in the sympathetic nervous system and is also significant for forming memories (Sasikumar, 2016). NE is crucial for the body’s stress response, regulating mood, attention and blood pressure. Similarly, cortisol, known as the stress hormone, mediates the body’s stress response and regulates the metabolism, inflammatory response and immune function (Thau, Gandhi & Sharma, 2023).
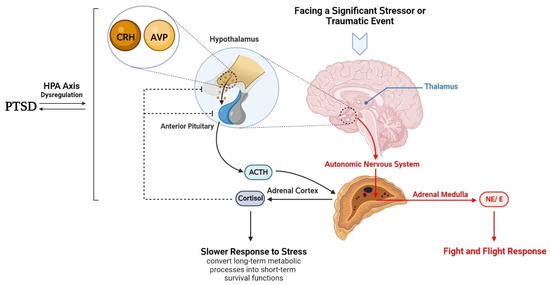
Figure 3: HPA axis dysregulation in post-traumatic stress disorder (Raise-Abdullahi et al., 2023).
Both of these messengers are released during a stress response, impacting the function of the hypothalamus. The hypothalamus further integrates the physiological aspects of the stress response, activating two neural systems: the autonomic nervous system (ANS) and the HPA axis. Upon activation, the ANS releases the hormone adrenaline as well as norepinephrine from the adrenal medulla, while the HPA axis releases glucocorticoids from the adrenal cortex, stimulating a cortisol-releasing response (Raise-Abdullahi et al., 2023).
These neurotransmitters are also involved in the process of encoding memories from a stressful event or emotionally salient memories. NE is an important modulator of memory, as it can regulate synaptic mechanisms; it is primarily released from the locus coeruleus in the brain. Emotional arousal leads to the activation of the locus coeruleus, which then results in NE release, further resulting in memory enhancement. NE activates both pre- and post-synaptic adrenergic receptors at central synapses, which have different functional outcomes depending on the type of receptor underlying distinct behavioural processes like memory. Research conducted by Tully and Bolshakov (2010) showed the effect of NE on memory. They treated rats systematically with the GABAA receptor antagonist picrotoxin to enhance their memory. Results showed a substantial increase in levels of NE within the amygdala. Following this, rats were also treated with GABAA receptor agonist muscimol, decreasing memory and subsequently the levels of NE. The varying levels of NE were modelling the acquisition of a conditioned fear memory, extensively showing that drugs are capable of modulating emotional memory, such as GABA agonists and antagonists, controlling levels of NE in the amygdala. Other findings included that injecting NE to various brain regions at times when memories are being encoded, or shortly after, could enhance memory performance. Conversely, decreased levels of NE could have detrimental effects on NE.
From this research, it is plausible to say that NE has a direct relationship with emotional memory and is a key player in memory consolidation for that reason (Tully & Bolshakov, 2010). Cortisol may also have a significant impact on memory encoding through its direct action on the hippocampal long-term potentiation. The release of cortisol can be seen to exhibit both memory-enhancing and impairing properties (Kim & Diamond, 2002; Joëls et al., 2006). Similarly, cortisol-driven memory enhancement occurs by the direct action of glucocorticoids on the hippocampus, which, due to its high receptor density, is highly sensitive to glucocorticoids. This glucocorticoid action on the hippocampus can significantly increase memory-related oscillations in the medial temporal lobe, thus potentiating memory (Heinbockel et al., 2021).
2.2 Dysregulation of Chemical Messenger Systems in PTSD Patients
As mentioned earlier, various chemical messenger systems, including NE and cortisol, are known to be dysregulated in PTSD. This, in turn, can lead to issues with memory encoding and retrieval. Traumatic events that cause PTSD can stimulate the release of NE, along with epinephrine, and can cause an overconsolidation of memory for a stressful event. A traumatic event often induces heightened physiological arousal, which activates the sympathetic nervous system. Since NE release is strongly linked to arousal and stress responses, traumatic experiences trigger excessive NE release, particularly from the locus coeruleus and adrenal medulla. These overactive NE levels result in a deeply engraved traumatic memory that is clinically expressed in the form of intrusive recollections, flashbacks, repetitive nightmares and perhaps conditioned emotional responses. There is also a chance of a positive feedback loop forming. When an already consolidated traumatic memory is reexperienced, it can cause the release of more NE and epinephrine, further strengthening the memory traces and causing an even greater chance of subsequent intrusive recollections. Although remembering past memories is important so that one can protect oneself from a similar situation in the future, this excess in NE and overconsolidation is known to be very painful (Southwick et al., 1999).
While a temporary release of both cortisol and NE during an event can be seen to significantly enhance memory encoding (also known as flashbulb memories), research shows that constantly elevated levels, such as those seen in individuals with PTSD, can impair the memory encoding process. One reason for this could be attributed to the excessive production of cortisol, whereby chronically high levels of stress in individuals with PTSD exhaust the HPA axis. Another way in which excessive cortisol is theorised to impact memory encoding is due to a decreased number of glucocorticoid receptors in PTSD, which contributes to higher levels of circulating cortisol in the bloodstream (Delaney, 2010). Further research suggests that high levels of stress hormones correlate with decreased activation in limbic areas, including the hypothalamus, medial orbitofrontal cortex, anterior cingulate cortex and the hippocampus. In addition to this, various behavioural and neuroimaging studies provide evidence to support the notion that glucocorticoid action exerts opposing effects on memory consolidation and retrieval due to the resulting decrease in hippocampal volume in PTSD compared to average (Wingenfeld & Wolf, 2014).
2.3 Learning in PTSD Patients
Research also shows that along with memory problems come learning issues for patients with PTSD. For example, in recent studies, it has been noticed that stress can cause NE release from the locus coeruleus, leading to increased spontaneous firing in the basolateral amygdala. This causes impaired extinction learning, which is the ability to form non-fearful associations. In order to treat patients, systematic and localised administration of propranolol could restore normal extinction learning (Giustino et al., 2020).
3. ADHD and PTSD: Different Roots of Episodic Memory Impairment
While memory impairment is a feature of PTSD, it is also a prominent characteristic of ADHD; however, the underlying mechanisms differ. Like PTSD, ADHD relies on norepinephrine, but also involves dopamine, a neurotransmitter related to motivation, attention and memory (Calabresi et al., 2007; Mehta et al., 2019). In ADHD, dysfunction is most notable in the prefrontal cortex (PFC), the brain region responsible for high-order executive functioning (Arneston, 2010; Goyal et al., 2008). Dopamine dysregulation in the PFC occurs in ADHD, meaning that individuals face challenges with attention and encoding information. On the other hand, individuals with PTSD struggle with memory impairments due to overactivation of the limbic system, causing weak and disorganised neutral memories. This distinction emphasises how episodic memory is impaired differently across the two conditions.
Figure 4: Location of the PFC in the brain (Psych Scene Hub, n.d.).
3.1 ADHD and Episodic Memory Aspects
The PFC is very sensitive to its neurochemical environment: either too much or too little catecholamine (stress) released in the PFC weakens cognitive control of behaviour and attention. Studies have shown that a blockade of A2 receptors, a stimulation that strengthens the functional connectivity of PFC networks, recreates the symptoms of ADHD, leading to impaired working memory (Brennan & Arnsten, 2008).
In ADHD, PFC dysfunction increases distractability, creating salient but irrelevant cues that fragment episodic memory and force the reliance on compensatory strategies like reminders (Platter & Bröder, 2012). Episodic memory can be fragmented into mechanisms like: temporal compression, when memories perform portions of events as if in “slices” (Ezzyat & Davachi, 2011); sleep deprivation, which weakens episodic associations (Ashton et al., 2011); and reconstructive retrieval, where gaps in memory are patched by schemes or inference. Fragmented memory in ADHD, worsened by salience and sleep disruption, weakens the episodic associations. Knowledge is then disjointed in slices, cumulative learning and retrieval of phrases of details (Ezzyat & Davachi, 2011; Ashton et al,. 2011).
3.2 PTSD and Episodic Memory Aspects
On the other hand, for people with PTSD, episodic memory is hampered because processes within effective recall strategies are disrupted. This could also relate to the emotional intensity of the traumatic experiences, which is contingent towards the impact on memory processes. Trauma-related emotional intensity causes the amygdala to become overactive while the hippocampus is suppressed, hindering memory recall; people with PTSD are not able to properly bind contextual details. By that, the episodic memories of traumatic events become fragmented, while frequently experienced as intrusive flashbacks rather than consistent recollections. These inconsistencies lead to negative impacts on the hippocampus and explain why people with PTSD do not have coherent, but rather emotion-based, experiences (Dickerson & Eichenbaum, 2010).
In addition, PTSD not only impacts traumatic memories but also impairs the process of recalling everyday episodic experiences. The exposure to chronic stress reduces the volume of the hippocampus, which is in charge of the connectivity and organisation process for memory over time. Tied with the impacts of intrusive flashbacks, the weakened connectivity mean people who experience PTSD also find it challenging to place ordinary events into a coherent timeline (Bremner, 2006).
3.3 Overlap and Misdiagnosis
ADHD and PTSD can both include similar overlapping traits, along with non-overlapping traits that present akin to each other. The overlapping traits that manifest in behaviour include difficulties in impulse control and heightened sensitivity towards sensory input, as well as emotional dysregulation, which includes symptoms of irritability, restlessness and anxiety.
However, despite the similarities in the symptoms of the disorders, the cognitive formation of episodic memories differs. Both ADHD and PTSD affect episodic memory, particularly difficulties in recalling and organising memories. In PTSD, intrusive memories are also present. Despite the similarities in cognitive affections, individuals with ADHD have a compensatory mechanism for the memory to form, as mentioned above, while individuals with PTSD have a difficult time forming and utilising the episodic memory.
As previously stated, because of the overlap in the symptoms, misdiagnoses between ADHD and PTSD can be common; correctly differentiating between them can be difficult as symptoms of traumatic stress can result in fidgeting and restlessness, which can often be seen as a symptom of ADHD. This is highlighted in Shi et al.’s research, where 30% of individuals with PTSD showed ADHD symptoms in their childhood, compared to only 11% of adults without a PTSD diagnosis (Shi et al., 2012).
Misdiagnosis between ADHD and PTSD can lead to the wrong forms of support and treatment. While some studies indicate stimulant medication, usually used to treat ADHD, could also be effective for PTSD (Baker & Moore, 2021), especially the memory and concentration aspects, stimulants are not yet approved as a treatment for PTSD. The primary medications used for PTSD are SSRIs, which have less basis as a treatment for ADHD; some studies even suspect SSRIs could further lower dopamine (Bremner, 2006). Therapeutic practices also vary between ADHD and PTSD.
4. Discussion and Conclusion
Identifying the extent to which chemical messenger dysfunction impacts memory in individuals with PTSD can aid in future research and therapeutic intervention within PTSD. Similar dysfunctions are also observed in disorders such as ADHD, where impairments in episodic memory have been linked to norepinephrine signalling, which suggests a potential shared pathway with PTSD. This is particularly important given that memory impairments in PTSD frequently extend beyond trauma recollections; they usually affect daily learning, decision making and quality of life in general. Possible research directions in the future should predominantly identify the interlinked complex neural pathways, hormones and neurotransmitters involved in the resulting memory deficits in PTSD, including longitudinal studies of the combined effects of both cortisol and NE in the brain, as well as more in-depth research emphasising the individual alterations in limbic and prefrontal brain regions in individuals with PTSD.
Highly detailed studies conducted on human-based models have been able to provide similar evidence as to the role of NE and cortisol on memory in PTSD. Multiple human studies with different types of trauma, populations and cultures could also provide more information about the role of NE and cortisol on memory in PTSD. This data triangulation signifies high reliability in the results, suggesting the research within this field can be directly applicable to various human populations. However, human-based models for research are very limited. Comparisons with ADHD research could provide further insights regarding how both disorders show disrupted episodic memory processes; ADHD studies have yet to increasingly emphasise the importance of human-based models. Furthermore, research regarding the impact of cortisol can be seen to be extensively and thoroughly studied on humans, providing highly detailed and specific evidence in this field, further strengthening the research on the impact of chemical messengers on memory in PTSD. In contrast, the role of the NE is still underexplored for human subjects, with most findings yet extrapolated from animal studies. This highlights the need for more large-scale, standardised human research that directly compares cortisol and NE for further investigation on the impact that memory dysfunction has on PTSD.
Whilst current research in this field is progressing, it can be argued to pose significant limitations impacting the general credibility of the data. The limited research conducted on the impact of NE on memory dysfunction in PTSD is seen to be predominantly conducted on rats, with very few studies conducted on humans. A minor amount of human-based studies are seen to lack standardised procedures, with the research methods showcasing significant variety in gender, past illnesses and other factors that otherwise result in differences in the procedure of the study, ultimately suggesting such research may be limited in the validity of its findings on human memory. In addition to this, the vast majority of the research is strictly conducted on animals. This animal model use may lack generalisability to human behaviour and brain systems, significantly limiting the applicability of such research on human memory. Moreover, small sample sizes and inconsistencies in the tools used to measure memory further reduce the strength of the conclusion. These methodological weaknesses limit the reliability and validity of the findings; the results may not properly portray real-world PTSD experiences. To address this, future researchers should prioritise consistent large-scale human studies while controlling health-related variables.
Comprehensively, these limitations highlight the gap between experimental findings and how they do not properly transfer into clinical practice. Regarding future research, human-based NE studies could aid in understanding its impact on the human brain exclusively, in particular when focusing on the combined impact of cortisol and NE on human memory in individuals with PTSD. In addition to this, medical intervention-based research can further look into the ways in which current and new therapeutic interventions can aid memory and learning in PTSD, instead of solely focusing on the underlying mechanisms of fear learning. Furthermore, this can be tied to the lack of research on various types of memory impacted by PTSD. Memory types such as long-term memory, procedural or working memory lack representation in research and may each be impacted differently by cortisol and NE in PTSD. Particularly for episodic memory, a type of long-term memory that allows individuals to recall specific events, is also often compromised in PTSD, similar to ADHD. Future research should consider directly contrasting these disorders to identify whether cortisol and NE influence episodic memory, in which ways and whether they are similar or distinct. By clarifying how each type of memory is uniquely disrupted, researchers could better inform therapeutic strategies. This would help to tailor interventions specific to the cognitive deficits. Understanding how each distinct memory type can be affected by both hormones and neurotransmitters in PTSD may be a crucial aspect of future research to focus on in this field, as it can allow for future modification of psychotherapeutic intervention in PTSD to accommodate the type of intervention to each specific individual case, which may ultimately provide the most efficiency to PTSD treatment methods.
In conclusion, the disruption of episodic memory present in PTSD can be attributed to the chemical messenger dysregulation, with resulting particular misdiagnosis in ADHD and PTSD due to the high comorbidity of both disorders. This further contributes to significant learning difficulties that further impact memory encoding.
Bibliography
Bandura, A. (1963). Social reinforcement and behavior change—Symposium, 1962: 1. Behavior theory and identificatory learning. American Journal of Orthopsychiatry, 33(4), pp. 591–601.
Bates, M. (2015a). Bullying and the Brain. [online] Brainfacts.org. Available at: https://www.brainfacts.org/thinking-sensing-and-behaving/childhood-and-adolescence/2015/bullying-and-the-brain.
Bates, M. (2015b). Bullying and the Brain. [online] www.sfn.org. Available at: https://www.sfn.org/sitecore/content/home/brainfacts2/thinking-sensing-and-behaving/childhood-and-adolescence/2015/bullying-and-the-brain.
Biederman, J., Petty, C.R., Spencer, T.J., Woodworth, K.Y., Bhide, P., Zhu, J. & Faraone, S.V. (2012). Examining the nature of the comorbidity between pediatric attention deficit/hyperactivity disorder and post-traumatic stress disorder. Acta Psychiatrica Scandinavica, 128(1), pp.78–87.
Carvalho, M., Branquinho, C. & De Matos, M.G. (2020). Cyberbullying and bullying: Impact on psychological symptoms and well-being. Child Indicators Research, 14(1).
Chen, Z., Zhang, J., Zhang, T., Zhang, F., Liu, Y., Ma, Y., Chen, Y. & Zhou, Z. (2025). The relationship between early adolescent bullying victimisation and suicidal ideation: the longitudinal mediating role of self-efficacy. BMC Public Health, 25(1).
Connaughton, M., Mitchell, O., Cullen, E., O’Connor, M., Banaschewski, T., Barker, G., Arun LW Bokde, Bruhl, R., Sylvane Desrivieres, Flor, H., Garavan, H., Gowland, P.A., Grigis, A.A., Heinz, A., Lemaitre, H., Jean-Luc Martinot, Marie-Laure Paillere Martinot, Artiges, E., Nees, F. & Orfanos, D.P. (2024). Bullying and Early Brain Development: A Longitudinal Structural Magnetic Resonance Imaging Study from Adolescence to Early Adulthood. bioRxiv (Cold Spring Harbor Laboratory). doi:https://doi.org/10.1101/2024.09.11.611600.
Conway, M.A. (2009). Episodic memories. Neuropsychologia, 47(11), pp. 2305–2313.
Cubillo, A. (2022). Neurobiological correlates of the social and emotional impact of peer victimisation: A review. Frontiers in Psychiatry, 13.
Delaney, E. (n.d). The Relationship between Traumatic Stress, PTSD and Cortisol. [online] Available at: https://upload.wikimedia.org/wikipedia/commons/0/0a/The_Relationship_between_Traumatic_Stress%2C_PTSD_and_Cortisol_%28IA_ptsd-and-cortisol-051413%29.pdf .
Ding, J., Lin, Y. & Chen, I-H. (2025). Why individuals with trait anger and revenge motivation are more likely to engage in cyberbullying perpetration? The online disinhibition effect. Frontiers in Public Health, 13.
Du Plessis, M.R., Smeekens, S., Cillessen, A.H.N., Whittle, S. & Güroǧlu, B. (2019). Bullying the Brain? Longitudinal Links Between Childhood Peer Victimisation, Cortisol, and Adolescent Brain Structure. Frontiers in Psychology, 9.
Elviira, P., Lindberg, M., Juho Härkönen, Scheinin, N.M., Karlsson, L., Karlsson, H. & Ekholm, E. (2023). Childhood trauma and fear of childbirth: findings from a birth cohort study. Archives of women’s mental health, 26(4), pp. 523–529.
Englander, E., Donnerstein, E., Kowalski, R., Lin, C.A. & Parti, K. (2017). Defining Cyberbullying. Pediatrics, [online] 140(Supplement 2), pp. S148–S151. doi:https://doi.org/10.1542/peds.2016-1758u.
Gini, G. & Pozzoli, T. (2013). Bullied Children and Psychosomatic Problems: A Meta-analysis. Pediatrics, [online] 132(4), pp. 720–729.
Giustino, T.F., Ramanathan, K.R., Totty, M.S., Miles, O.W. & Maren, S. (2020). Locus Coeruleus Norepinephrine Drives Stress-Induced Increases in Basolateral Amygdala Firing and Impairs Extinction Learning. Journal of Neuroscience, 40(4), pp. 907–916.
González-Cabrera, J., Calvete, E., León-Mejía, A., Pérez-Sancho, C. & Peinado, J.M. (2017). Relationship between cyberbullying roles, cortisol secretion and psychological stress. Computers in Human Behavior, 70, pp.153–160.
Google Books. (2025). Neuropsychology of PTSD. [online] Available at: https://books.google.co.uk/books?hl=en&lr=&id=WW6bmGCzHvEC&oi=fnd&pg=PA131&dq=normal+memory+encoding+vs+ptsd+memory+encoding&ots=AxkZtnl6VZ&sig=g190i008ieK-VSwcy8eFEIDncME#v=onepage&q=memory&f=false.
John, A., Glendenning, A.C., Marchant, A., Montgomery, P., Stewart, A., Wood, S., Lloyd, K. & Hawton, K. (2018). Self-Harm, Suicidal Behaviours, and Cyberbullying in Children and Young People: Systematic Review. Journal of Medical Internet Research, 20(4), p.e129.
Johnson, J. (2021). Topic: Cyber bullying. [online] www.statista.com. Available at: https://www.statista.com/topics/1809/cyber-bullying/.
Juvonen, J. & Graham, S. (2014). Bullying in Schools: The Power of Bullies and the Plight of Victims. Annual Review of Psychology, 65(1), pp.159–185.
Juvonen, J., Wang, Y. & Espinoza, G. (2010). Bullying Experiences and Compromised Academic Performance Across Middle School Grades. [online] ResearchGate. Available at: https://www.researchgate.net/publication/241653629_Bullying_Experiences_and_Compromised_Academic_Performance_Across_Middle_School_Grades.
Kasturiratna, K.T.A.S., Hartanto, A., Chen, C.H.Y., Tong, E.M.W. & Majeed, N.M. (2024). Umbrella review of meta-analyses on the risk factors, protective factors, consequences and interventions of cyberbullying victimisation. Nature Human Behaviour. [online] doi:https://doi.org/10.1038/s41562-024-02011-6.
Ke, T., De Simoni, S., Barker, E. & Smith, P. (2022). The association between peer‐victimisation and structural and functional brain outcomes: A systematic review. JCPP Advances, 2(2).
Kowalski, R.M., Giumetti, G.W., Schroeder, A.N. & Lattanner, M.R. (2014). Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychological Bulletin, 140(4), pp.1073–1137.
Lee, K.H., Yoo, J.H., Lee, J., Kim, S.H., Han, J.Y., Hong, S.-B., Shin, J., Cho, S.-C., Kim, J.-W. & Brent, D.A. (2020). The indirect effect of peer problems on adolescent depression through nucleus accumbens volume alteration. Scientific Reports, 10(1).
Manuel, B. (2023). 16 Cyberbullying Statistics, Facts & Trends for 2023. [online] Cloudwards. Available at: https://www.cloudwards.net/cyberbullying-statistics/.
Mbah, R. (2020). The Perception of Students About School Bullying and How It Affects Academic Performance in Cameroon [thesis]. Available at: https://memorial.scholaris.ca/server/api/core/bitstreams/fbf6dd97-2303-4ab7-9a71-e30180849d1c/content.
McLaughlin, K.A., Colich, N.L., Rodman, A.M. & Weissman, D.G. (2020). Mechanisms linking childhood trauma exposure and psychopathology: a transdiagnostic model of risk and resilience. BMC Medicine, 18(1), pp.1–11.
McLoughlin, L.T., Shan, Z., Broadhouse, K.M., Winks, N., Simcock, G., Lagopoulos, J. & Hermens, D.F. (2019). Neurobiological underpinnings of cyberbullying: A pilot functional magnetic resonance imaging study. Human Brain Mapping. [online] doi:https://doi.org/10.1002/hbm.24890.
McLoughlin, L.T., Shan, Z., Mohamed, A., Boyes, A., Driver, C., Lagopoulos, J. & Hermens, D.F. (2022). Gender differences in brain activity when exposed to cyberbullying: Associations between wellbeing and cyberbullying experience using functional Magnetic Resonance Imaging. Current Research in Neurobiology, 3, p.100054.
Mulenga, K.M., Kakupa, P. & Xia, L.-X. (2025). Implications of Bullying Victimisation on Mental Health Among Male Juvenile Offenders Within a Reformatory Facility in Zambia. Journal of interpersonal violence, [online] p.8862605251339639. doi:https://doi.org/10.1177/08862605251339639.
ONS (2021). Home – Office for National Statistics. [online] Ons.gov.uk. Available at: https://www.ons.gov.uk.
Palamarchuk, I.S. & Vaillancourt, T. (2022a). Integrative Brain Dynamics in Childhood Bullying Victimisation: Cognitive and Emotional Convergence Associated With Stress Psychopathology. Frontiers in Integrative Neuroscience, 16.
Parga, A.D. & Liska, T.M. (2025). Stigma, Bullying, and Resilience: Psychosocial Outcomes in Marginalized Adolescents With Visible Dermatologic Conditions. Cureus. [online] doi:https://doi.org/10.7759/cureus.86171.
Peled, Y. (2019). Cyberbullying and its influence on academic, social, and emotional development of undergraduate students. Heliyon, 5(3), p.e01393.
Perino, M.T., Guassi Moreira, J.F. & Telzer, E.H. (2019). Links between adolescent bullying and neural activation to viewing social exclusion. Cognitive, Affective, & Behavioral Neuroscience, 19(6), pp.1467–1478.
Prince, T., Driver, C., Boyes, A., Mulgrew, K.E., Elwyn, R., Mills, L. & Hermens, D.F. (2025). The neural underpinnings of body image-related cyberbullying in adolescent females: A proposed neurobiological model. Behavioural Brain Research, pp.115647–115647.
PsycNet (n.d.). APA PsycNet. [online] Available at: https://psycnet.apa.org/record/2010-04134-003.
Raise-Abdullahi, P., Meamar, M., Vafaei, A.A., Alizadeh, M., Dadkhah, M., Shafia, S., Ghalandari-Shamami, M., Naderian, R., Afshin Samaei, S. & Rashidy-Pour, A. (2023). Hypothalamus and Post-Traumatic Stress Disorder: A Review. Brain Sciences, [online] 13(7), p.1010.
Renzo Abregú-Crespo, Garriz-Luis, A., Ayora, M., Nuria Martín-Martínez, Cavone, V., Ángel, M., Fraguas, D., Martín‐Babarro, J., Arango, C. & Díaz‐Caneja, C.M. (2023). School bullying in children and adolescents with neurodevelopmental and psychiatric conditions: a systematic review and meta-analysis. The Lancet Child & Adolescent Health, 8(2).
Rivara, F., Adhia, A., Lyons, V., Massey, A., Mills, B., Morgan, E., Simckes, M. & Rowhani-Rahbar, A. (2019). The Effects Of Violence On Health. Health Affairs, 38(10), pp.1622–1629.
Rivara, F. & Menestrel, S.L. (eds) (2016a). Consequences of Bullying Behavior, Preventing Bullying Through Science, Policy, and Practice. [online] Available at: https://www.ncbi.nlm.nih.gov/books/NBK390414.
Schienle, A. & Scharmüller, W. (2013). Cerebellar activity and connectivity during the experience of disgust and happiness. Neuroscience, 246, pp.375–381.
Shah, R., Dodd, M., Allen, E., Viner, R. & Bonell, C. (2022). Is being a victim of bullying or cyberbullying in secondary school associated with subsequent risk‐taking behavior in adolescence? A longitudinal study in secondary schools. Journal of Adolescence, 94(4), pp.611–627.
Sherman, B.E., Harris, B.B., Turk‐Browne, N.B., Sinha, R. & Goldfarb, E.V. (2023). Hippocampal mechanisms support cortisol-induced memory enhancements. The Journal of Neuroscience, 43(43), p.JN-23.
Simmons, K.X., Shah, N.N., Fakeh Campbell, M.L., Gonzalez, L.N., Jones, L.E. & Shendell, D.G. (2020). Online and in‐Person Violence, Harassment, Intimidation and Bullying in New Jersey: 2011‐2016. Journal of School Health, 90(10), pp.754–761.
Smith, P.K., Mahdavi, J., Carvalho, M., Fisher, S., Russell, S. & Tippett, N. (2008). Cyberbullying: its nature and impact in secondary school pupils. Journal of child psychology and psychiatry, and allied disciplines, 49(4), pp.376–385.
Southwick, S.M., Bremner, J.Douglas., Rasmusson, A., Morgan, C.A., Arnsten, A. & Charney, D.S. (1999). Role of norepinephrine in the pathophysiology and treatment of posttraumatic stress disorder. Biological Psychiatry, 46(9), pp.1192–1204.
Statista. (2023). Discord actioned content by category 2023. Statista. [online] Available at: https://www.statista.com/statistics/1284183/discord-user-reports-actioned-by-category/.
Takizawa, R., Maughan, B. & Arseneault, L. (2014). Adult Health Outcomes of Childhood Bullying Victimisation: Evidence From a Five-Decade Longitudinal British Birth Cohort. American Journal of Psychiatry, 171(7), pp.777–784.
Tessner, K.D., Walker, E.F., Dhruv, S.H., Hochman, K. & Hamann, S. (2007). The relation of cortisol levels with hippocampus volumes under baseline and challenge conditions. Brain Research, 1179, pp.70–78.
Thau, L., Gandhi, J. & Sharma, S. (2023). Physiology, Cortisol. [online] Nih.gov. Available at: https://www.ncbi.nlm.nih.gov/sites/books/NBK538239/
Tokunaga, R.S. (2010). Following you home from school: A critical review and synthesis of research on cyberbullying victimisation. Computers in Human Behavior, 26(3), pp.277–287.
Tully, K. & Bolshakov, V.Y. (2010). Emotional enhancement of memory: how norepinephrine enables synaptic plasticity. Molecular Brain, 3(1), p.15.
Vaillancourt, T. (2025). The Neurobiology of Bullying Victimisation. The Cambridge Handbook of Violent Behavior and Aggression, pp.175–186.
Van Geel, M., Vedder, P. & Tanilon, J. (2014). Relationship Between Peer Victimisation, Cyberbullying, and Suicide in Children and Adolescents. JAMA Pediatrics, 168(5), p.435.
Vogels, E.A., Gelles-Watnick, R. & Massarat, N. (2022). Teens, social media and technology 2022. Pew Research Center. [online] Available at: https://www.pewresearch.org/internet/2022/08/10/teens-social-media-and-technology-2022/.
Waasdorp, T.E. & Bradshaw, C.P. (2015). The Overlap Between Cyberbullying and Traditional Bullying. Journal of Adolescent Health, 56(5), pp.483–488.
Wetherall, K., Robb, K.A. & O’Connor, R.C. (2019). Social rank theory of depression: A systematic review of self-perceptions of social rank and their relationship with depressive symptoms and suicide risk. Journal of Affective Disorders, 246, pp.300–319.
Wilson, N. & Sun, R. (1984). Coping with Bullying: A Computational Emotion-Theoretic Account. [online] Available at: https://escholarship.org/content/qt11w8r47j/qt11w8r47j_noSplash_ff55706687582baeaca9a274dcf65b2a.pdf?t=op9xya
Wilton, C., Campbell, M. & Prof, A. (2016). An exploration of the reasons why adolescents engage in traditional and cyber bullying. [online] Available at: https://eprints.qut.edu.au/47912/1/47912A.pdf.
Yang, Y., Jimmy, J., Jones, E.E., Kreutzer, K.A., Bryan, C.J. & Gorka, S.M. (2023). Neural reactivity to threat impacts the association between bullying victimisation and suicide risk in youth. Journal of Psychiatric Research, 163, pp.288–295.
Yebra, M., Galarza-Vallejo, A., Soto-Leon, V., Gonzalez-Rosa, J.J., De Berker, A.O., Bestmann, S., Oliviero, A., Kroes, M.C.W. & Strange, B.A. (2019). Action boosts episodic memory encoding in humans via engagement of a noradrenergic system. Nature Communications, 10(1).
Ying, H. & Han, Y. (2024). How childhood psychological abuse affects adolescent cyberbullying: The chain mediating role of self-efficacy and psychological resilience. PLoS ONE, 19(9), pp.e0309959–e0309959.
Zahn, R., Moll, J., Krueger, F., Huey, E.D., Garrido, G. & Grafman, J. (2007). Social concepts are represented in the superior anterior temporal cortex. Proceedings of the National Academy of Sciences, 104(15), pp.6430–6435.
Zhao, N., Yang, S., Zhang, Q., Wang, J., Xie, W., Tan, Y. & Zhou, T. (2024). School bullying results in poor psychological conditions: evidence from a survey of 95,545 subjects. Frontiers in psychology, 15.




{kind=link}