
Table of Contents
– 1. Introduction
– 2. The Role of Personality Traits in Adverse Childhood Experiences
– – 2.1 Parenting Styles and Cultural Differences
– – 2.2 Types of Parenting Styles
– – 2.3 Intergenerational Aspects
– 3. Prolonged Trauma: The Aftermath of Adverse Childhood Experiences
– – 3.1 The Spectrum of PTSD: Categories and Impacts
– – 3.2 Adverse Childhood Experiences in Children
– – 3.3 Impact of Adverse Childhood Experiences on Social Functioning
– 4. Lifespan Progression of PTSD Following Adverse Childhood Experiences
– 5. Prevention and Mitigation of Adverse Childhood Experiences and PTSD
– 6. Discussion
1. Introduction
Trauma, derived from the Greek word “τραῦμα” for “wound” or “hurt”, is defined as an experience subjectively perceived as distressing or painful (Feriante & Sharma, 2023). Trauma itself was studied in the late 19th century when “hysteria” was diagnosed in subjects who were able to relive their past subjective experiences (Van der Kolk, 2000). Following further studies of trauma, Kardiner played a crucial role in the “rediscovery” of trauma in a subjective and psychological sense in the form of Post-Traumatic Stress Disorder (PTSD), which was founded through the methods of diagnosing severely traumatised individuals involved in war crime, including the Vietnam War, in which the Diagnostic and Statistical Manual of Mental Disorders (DSM) was published (Friedman, 2025). Although approximately 70% of the world’s population experiences a traumatic event in their lifetime in some form or another, only 3.9% of them will develop PTSD. Individuals with PTSD experience involuntary recollection of the subjected traumatic events, resulting in avoidant behaviours so as not to trigger these memories, and often face symptoms of hyperarousal (World Health Organization, 2024).
Trauma is subjective and can occur at any phase of an individual’s life. Trauma and abuse at an early age can dysregulate a child’s neurobiological system, reducing their resistance to stressful or emotional events and leading to prolonged difficulties with emotional regulation. This is particularly relevant for young individuals who have faced physical or emotional abuse as their perceived view of safety depends on their attachment figures (National Child Traumatic Stress Network, 2023). This often results in the child exhibiting increased hypersensitivity to signs of anger or threat in their environment (Giotakos, 2020). Following this, in the emotionally critical age of adolescence, PTSD is common and debilitating, and while most research has focused on adults, growing attention is given to its impact on youth (Tamir et al., 2025). 18.8% of youth are exposed to trauma, with numbers up to 40% in abuse and assault cases. Due to the onset of puberty in adolescence, the emotional and hormonal instability leads to an increased risk of developing PTSD in the future (Cisler & Herringa, 2021). Given the heightened vulnerability of adolescents to trauma and its lasting psychological impact, understanding the specific diagnostic criteria for PTSD is essential to identify and address these symptoms effectively (NIMH, 2023; Mind, 2023).
The current research clearly displays an interrelation between adverse childhood experiences (ACEs) and the presence of PTSD in later stages of life. This research paper will primarily focus on the influence of parenting characteristics. Additionally, we discuss the effects of ACEs on growing individuals, including neurobiological implications. Furthermore, our research aims to provide measures for those affected by trauma, mitigate the effect of relapses and help individuals feel more comfortable and confident in society.
2. The Role of Personality Traits in Adverse Childhood Experiences
2.1 Parenting Styles and Cultural Differences
Parents’ personality traits produce enduring psychological effects on children, which are further influenced by cultural context. Baumrind identified three primary parenting styles: permissive, authoritarian and authoritative.
Permissive parenting is characterised by overt warmth and acceptance, minimal demands for responsibility, extensive consultation with the child and near-complete avoidance of control. This style fosters autonomy but often does not possess any structure, discipline or external guidance (Baumrind, 1966). However, this parenting style usually involves the parent viewing their child as uniquely special, accompanied by a general pattern of indulgence. This perspective may foster entitlement; for example, the child internalising a sense of superiority and expecting constant attention. Over time, this may hinder emotional maturity, impair the development of healthy relationships and increase the risk of low frustration tolerance, poor anger regulation and narcissistic tendencies in adulthood (Little, 2024).
Authoritarian parenting seeks to shape and control the child’s behaviour according to strict, often absolute, standards. Obedience is highly valued, autonomy is restricted and household responsibilities are assigned to instil discipline and respect for structure. Dialogue is limited, with the parent expecting unquestioned compliance with their directives (Baumrind, 1966). However, authoritarian parenting shows the highest correlation with child aggression (Muhammad et al., 2022). Additionally, when such parents engage in derisive parenting – behaviours that demean or belittle – adolescents are more likely to exhibit dysregulated anger, which can contribute to increased bullying and victimisation (Dickson et al., 2019).
Authoritative parenting guides a child’s behavior in a rational, issue-oriented manner, balancing firm direction with respect for the child’s autonomy. Parents encourage dialogue, explain the reasoning behind rules and consider the child’s objections. Both self-will and disciplined conformity are valued, with firm but reasonable control, affirmation of the child’s qualities and clear standards for future conduct (Baumrind, 1966). According to Baumrind, children of authoritative parents develop good social skills, are self-confident about their abilities to learn new things, have good emotional regulation and tend to have happier dispositions as opposed to their peers (Kuppens & Ceulemans, 2019). Research suggests that authoritative parenting is associated with better creativity, life satisfaction, problem-solving abilities, high self-esteem and self-confidence. While authoritative parenting is often viewed as the most effective approach, it is recognised that various factors play a role in developmental outcomes (Lau & Power, 2019).
It is important to note that cultural differences largely influence parenting traits. Researchers have clearly distinguished the biggest cultural difference between Western and Eastern types of parenting mindsets. Hofstede found that Western families typically have a lower power-distance relationship between child and parent, whereas Eastern families tend to have a high power-distance relationship.
In low power-distance relationship cultures, children are encouraged to question and negotiate, with parents creating an environment of democratic decision-making and providing explanations for rules (Hofstede, 2001). Research comparing parent-adolescent communication across cultures shows that Western, low–power-distance societies (such as Sweden, the U.S. and parts of Western Europe) typically encourage open dialogue, negotiation and the questioning of parental authority (Alampay & Rothenberg, 2020). This highlights that this communicative style is not merely a preference but a culturally embedded expectation, shaping how adolescents interpret warmth, autonomy and parental legitimacy. Their findings demonstrate that in these contexts, democratic communication is linked to healthier emotional internalising and reduced symptoms over time.
Contrary to the above, Ruth Chao showed that what Western psychology labels “authoritarian” is better understood in Chinese families as “chiao shun” or “training”: high involvement, high academic expectations and strictness as a sign of care and investment. This is not associated with the same negative connotations present in Western contexts (Chao, 1994). In Middle Eastern and North African cultures, studies show that parental authority reflects cultural roles. Strictness is seen as maintaining family cohesion and moral responsibility, and children interpret control as protective rather than punitive (Kagitcibasi, 2017). Similarly, African American families usually have a “no-nonsense” parenting style, where high control and high warmth is interpreted as safety in hostile environments (Brody & Flor, 1998).
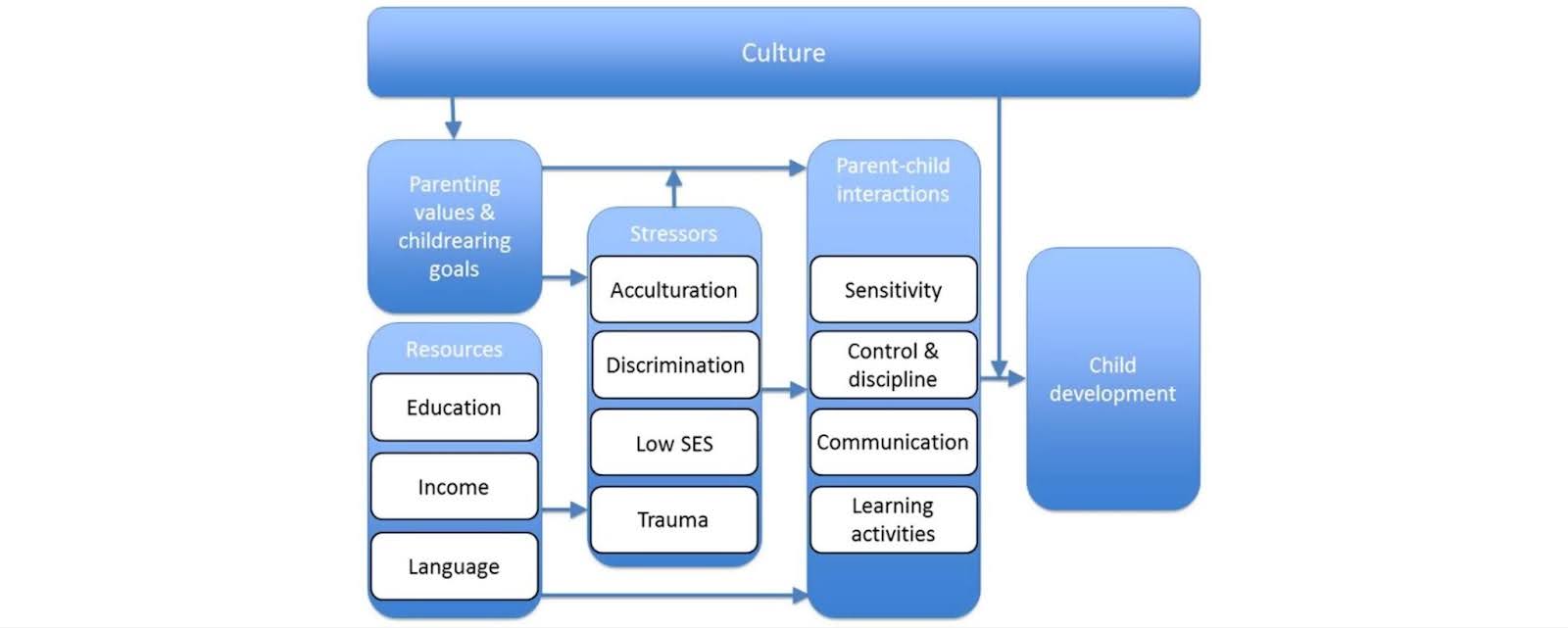
Role of Cultural Differences in Parenting Styles (Prevoo & Tamis-LeMonda, 2017).
[Abbreviations: SES = socioeconomic status].
2.2 Types of Parenting Styles
The term “helicopter parenting” was first introduced in 1990 to describe the way parents metaphorically “hover” over their children in an effort to spare them from disappointment and pain. By doing so, they are teaching their children that they are unable to “rescue” themselves in times of struggle. By violating their children’s need for competence and autonomy, helicopter parents foster heightened levels of anxiety and depression. By being overprotective, parents reinforce a sense of danger, leading children to perceive challenges as potential threats (Vigdal & Brønnick, 2022). Helicopter parents also have the tendency to impose unrealistic standards on their children in order to create a perfect image for the outside world. When this is combined with the child’s already low sense of efficacy, the chances of developing depression and anxiety increase. A low sense of efficacy increases feelings of futility. Consequently, individuals who do not believe they can sufficiently contribute with their actions to reach a desired outcome will not feel they have a reason to persevere in the face of the challenges they meet (Vigdal & Brønnick, 2022).
Parentification, also referred to as adultification or role-reversal, occurs when children are forced to assume adult-like responsibilities. Parentified children become pseudo-adults long before they possess the cognitive or physiological capacity to assume such roles (Dariotis et al., 2023). Parentification can serve multiple functions. Instrumental parentification involves practical tasks necessary for maintaining a household, such as taking care of meals, finances or chores. Emotional parentification requires the child to regulate and support the emotional needs of the family, for example, mediating conflicts and maintaining harmony amongst family members. Based on the relationship in which the reversal occurs, parentification can be parent-focused (the child becomes the caregiver of their own parent), sibling-focused (the child assumes parental responsibilities for their siblings) or spouse-focused (the child becomes the parent’s confidant). Although parentification may lead to positive traits such as maturity or empathy, it is also linked to adverse life outcomes. Research shows that parentified children are at higher risk of depression, anxiety, drug use, addiction, poor physical health and unemployment (Dariotis et al., 2023). As adults, they might struggle with maintaining healthy relationships, setting boundaries, trusting others and emotional regulation.
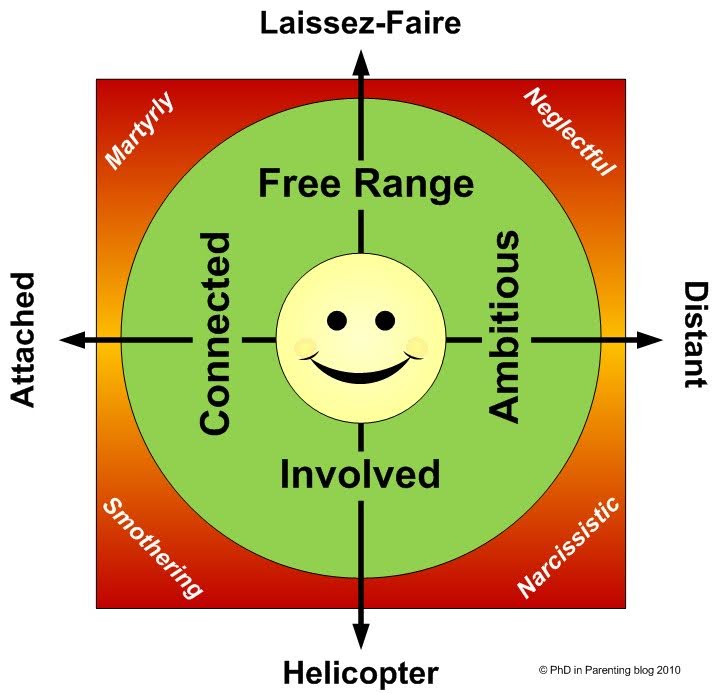
Parenting Styles (PhD in Parenting, 2016).
Bonds between narcissistic parents and their children are often strained, as these types of parents typically experience lower levels of satisfaction in the relationship. There are two major subtypes of narcissistic traits. Individuals with grandiose narcissism display an exaggerated sense of their own importance (Palumbo, 2023). Their behaviour is usually driven by their need for self-enhancement, i.e. the behaviour is designed to increase self-esteem (APA, 2018). Grandiose narcissists are extroverts and sometimes aggressive. Vulnerable narcissists, on the other hand, are more reserved in their narcissistic behaviours. They are self-absorbed, hypersensitive and defensive, but prone to social insecurity. Their defensiveness is caused by their own feelings of incompetence.
Although both types of parental narcissism result in negative effects in the adult child, vulnerable narcissism is the subtype that has the most effect. It is associated with adverse effects of low wellbeing, low self-esteem, adverse parenting styles and adverse attachment styles. Grandiose narcissism has also been linked with adverse parenting styles and adverse attachment styles, but no association with low self-esteem or wellbeing (Palumbo, 2023).
2.3 Intergenerational Aspects
The definition of child abuse and neglect (CAN) is physical, emotional or sexual abuse and/or neglect, as well as the witnessing of intimate partner violence (IPV) between parents, which may result in harm to a child’s health and perceptions of trust and power within a relationship. While IPV involves sexual or psychological abuse by a current or former intimate partner, this is the most common form of family violence. When children are exposed to CAN or IPV, they are more prone to a state of hyperarousal, which increases physiological and psychological tension. These children are at a higher risk of becoming subjected to IPV and CAN during adulthood. Furthermore, people who have suffered from CAN or IPV can also develop mental health problems, including PTSD, anxiety, depression and aggression (Assink et al., 2018).
There are numerous factors that contribute to child maltreatment, including: (1) parental and child-related factors; (2) family-related factors; (3) risk factors present in the community of the family and surrounding social system; and (4) risk factors regarding societal attitude towards children and abuse. Parental mental health problems, including experiencing stress, alcohol and drug abuse or low self-esteem, frequently translates into mental health problems in children, showcasing the vicious cycle of intergenerational trauma and mental health. A recent meta-analysis, conducted by Assinik et al. recorded that parents with a history of CAN are three times more likely to mistreat and abuse their children in comparison to a parent who has never experienced CAN (Assink et al., 2018).
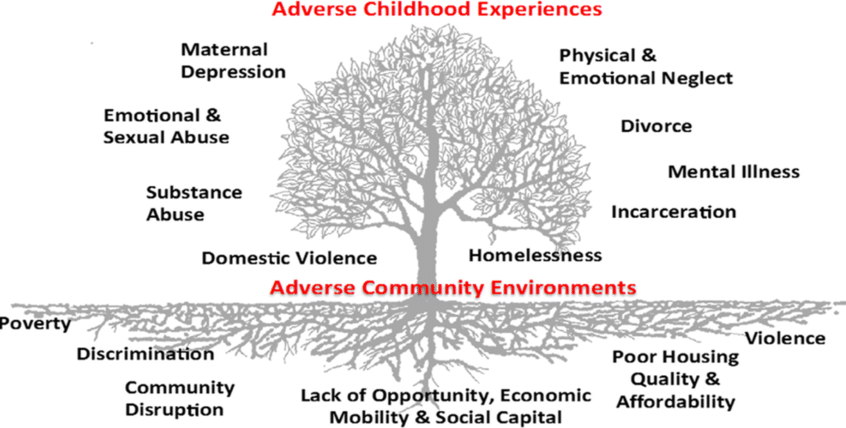
The Tree of ACEs (Ellis & Dietz, 2017).
3. Prolonged Trauma: The Aftermath of Adverse Childhood Experiences
In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), PTSD is defined by several characteristics grouped under seven major categories. This is crucial in understanding how we validate PTSD (Mureșanu et al., 2022). As we grow older, changes in our social or physical environments are common. The hippocampus, known for its strong neuroplasticity and regenerative capacity, helps us adapt to these modifications. Yet this same neuroplasticity can be affected by early trauma, which explains why the impact of ACEs may persist (Bremner, 2006). Trauma may be experienced briefly; however, its impacts are endured within an individual’s system until they have been acknowledged and treated (Guy-Evans, 2021).
3.1 The Spectrum of Trauma and PTSD: Categories and Impacts
Trauma is mainly divided into two categories – direct and indirect – which are distinct but can be interlinked in many ways. When an individual experiences trauma firsthand, this is known as direct trauma. Direct traumas, whether psychological or physiological, are more susceptible to persist for longer periods of time (American Psychological Association, 2025). In contrast, indirect trauma stems from learning about another person’s trauma.
“Witnessed trauma”, being one of the most experienced traumas by humans at 70%, is a prominent risk factor in the development of PTSD. Neuroactive steroids (NASs), which act as positive allosteric modulators (substances that enhance enzyme activity by binding to a secondary site), such as allopregnanolone, have been implicated in pathopsychology and explored as a treatment strategy for witnessed trauma-induced PTSD (Aidan Evans‐Strong et al., 2024). Another extremely relevant form of indirect trauma is vicarious trauma. Though not distinctly defined as a disorder, the DSM-V recognises vicarious trauma under “Criterion A”. Professionals in legal and judiciary industries experience this trauma on a much greater level compared to others (Scott & Freckelton, 2024).
The development of PTSD may occur following the immediate impact of the traumatic event or years after its advent. An individual is affected as they relive their experiences through nightmares and flashbacks. The impacts of PTSD cause severe and persistent symptoms that significantly affect an individual’s daily life (NHS, 2022). These impacts include symptoms such as: individuals experiencing somatisation, sleep disturbances, neurological and substance use disorders (SAMHSA, 2014). If an individual repeatedly experiences a traumatic event multiple times, they may develop Complex Post-Traumatic Stress Disorder (CPTSD) (American Psychological Association, 2025). Although PTSD is more commonly heard of, CPTSD is evidently diagnosed more often, as statistics for those meeting the criteria of CPTSD rose higher than PTSD in the ICD-11 (CPTSD 80%, PTSD 20%). Symptoms of CPTSD are relatively similar compared to PTSD; however, an additional cluster of dissociative symptoms, such as depersonalisation or derealisation, as well as regular suicidal feelings, are witnessed in CPTSD. Furthermore, individuals with CPTSD have an increased likelihood of displaying symptoms that reflect major depressive disorders as evidence samples suggest that CPTSD is commonly associated with Borderline Personality Disorder (BPD) (Murphy et al., 2021).
3.2 Adverse Chilhood Experiences in Children
The hippocampus is part of the brain’s structure, located in the medial temporal lobe and crucial for learning and memory. Vital hippocampal development first occurs during prenatal development. In an analysis, Seress et al. (2001) observed that during infancy, early stages of hippocampal development, the hippocampal cornu ammonis (CA) fields are partially more mature compared to the debate gyrus. Parallel to early hippocampal development is the rapid growth of memory; however, with the lack of empirical evidence, we struggle to establish a connection between early hippocampal development and the increase of such cognitive competencies. Gomez and Edwin (2015) and Lavenex and Banta Lavenex (2013) proposed that surfacing memory abilities can depend on the monosynaptic circuit, which could introduce the first basic forms of episodic memory (Lee, Johnson & Ghetti, 2017).
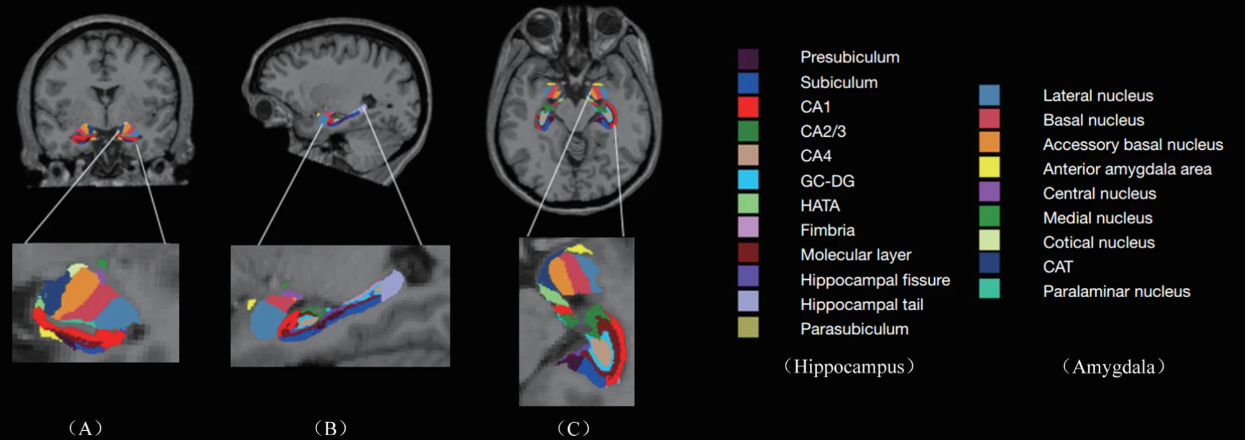
Automatic Segmentation of Hippocampus and Amygdala (Lu et al., 2024).
During early childhood, the brain goes through its most sensitive periods, forming over 1 million new neural connections per second (First Things First, 2018). Due to this, it becomes vulnerable to the effects of relationships, as well as other factors, which can disrupt normal cognitive and emotional development.
3.3 Impact of Adverse Childhood Experiences on Social Functioning
One’s social life can be drastically affected by ACEs. Studies show that people with social anxiety are also more likely to have experienced ACEs (Psychology Today, 2024). Similarly, physical health issues such as endocrine disorders, autoimmune disorders, chronic pain, cardiovascular issues and sleep disturbances are very common due to ACEs and can affect social functioning. Individuals frequently face emotional and behavioural consequences such as impulsivity, lack of trust, anxiety, low self-esteem, depression, substance abuse, aggression and self-harm (Catalyst Care Group, 2025).
4. Lifespan Progression of PTSD Following Adverse Childhood Experiences
ACEs have long-term effects as the body holds chronic stress, causing structural and functional changes in the brain, further influencing cognitive processes and emotional regulation. Chronic stress causes hyperactivity in the amygdala, reducing the volume of the prefrontal cortex (PFC) and decreasing the amount of neurogenesis in the hippocampus (Blum, 2024).
The lasting effects of ACEs range from numerous manifestations, specifically, psychological and physiological factors, which impact how individuals cope in healthy environments. The Adverse Childhood Experience Questionnaire (ACE-Q), conducted by Kaiser Permanete (Zarse et al., 2019b), conveys the overall increase of risks in individuals to develop psychological and physiological issues. During 1996, 13,494 patients completed the survey, leaving a 70.5% response sample, concluding that increased ACE scores were concurrent with a greater degree of adult illness burden. A study of 416 psychiatric patients reported that 31% of those experienced substantial pain. The subjective reports linked significant pain levels to higher ACE scores in women and men, the pain symptoms included: back pain; chronic pain; headaches and migraines (Greggersen et al., 2010). The long-term effects of ACEs, unfortunately, are not something an individual may “age out” of as adults above the age of 65 who were exposed to high levels of ACEs also struggle with personality disorders (Rapso, Henriksen & Afifi, 2014).
Furthermore, a comprehensive study conducted by the World Health Organization (WHO) reveals that ACEs have contributed significantly to the overall prevalence of mental disorders, accounting for 29.8% of cases worldwide (Greiner et al., 2025). Various studies found different psychological issues associated with individuals scoring high on the ACE-Q, including increased risks of developing PTSD (Corbin et al,. 2013), sleep disorders (Chapman et al., 2011) and suicide attempts, as well as increased cigarette use (Dube et al., 2003).
5. Prevention and Mitigation of Adverse Childhood Experiences and PTSD
In the prevention of ACEs, it is essential to address the conditions that cause adversity. Strategies preventing adversity will focus on adapting to normal environments and behaviours in order to prevent the recurrence of ACEs. This may include adaptations of schools instituting better counselling measures or adaptations of healthcare and mental health providers. Effectively reducing the number of ACEs requires communication and contribution between sectors such as governments, social services, public health and education (CDC, 2024b).
CAN and Responses (Han et al., 2024).
The Centres for Disease Control and Prevention (CDC) provides strategies which can be implemented to prevent/mitigate PTSD caused by ACEs. These aim to:
- Strengthen economic support to families by implementing improved policies.
- Ensure a strong start for children by authorising home-based support programmes.
- Teach people stress-handling skills, such as relationship and communication skills.
By systematic and technical use of these strategies, we can foster communities with reduced PTSD due to ACEs (CDC, 2024).
6. Discussion
Parents’ personality traits shape children’s emotional development through culturally embedded parenting styles. This paper has identified the traits of three distinctive parenting styles and shown how each of these channel particular characteristics into the child’s developing emotional and psychological state. The three primary types, including permissive, authoritative and authoritarian parenting styles, all differ from each other in control, warmth and communication, and produce different outcomes. Cultural context modifies these patterns, with Western, low–power-distance societies favouring democratic, dialogic parenting, whereas more collectivistic Eastern cultures often prioritise obedience and familial hierarchy overall. These culturally-embedded parenting styles influence children’s self-regulation, emotional security and long-term psychological outcomes and the type of person they eventually become in adulthood.
A parent’s approach to raising their child can negatively affect the child’s development. Certain traits of the parent can greatly influence their parenting style. Narcissistic parents have trouble maintaining a healthy relationship with their children, as they have low levels of satisfaction in this relationship. “Helicopter parenting” is a term that has been used for over 30 years and describes a parent’s overprotectiveness and unrealistic expectations which can lead to anxiety and depression. Another lesser-known phenomenon with the same outcomes is parentification, the reversal of roles between a parent and their child. A parent who has experienced CAN and IPV is three times more likely to mistreat their child than a parent who has never been exposed to such brutality in their household. The parent who has experienced this maltreatment may naturally become desensitised to it, perceiving it as normal and developing poor emotional regulation. They will then, in turn, be more likely to resort to poor coping mechanisms such as drugs and alcohol, repeating the vicious cycle of intergenerational trauma. Now the second generation of the family is also three times more likely to commit CAN and IPV.
The DSM-V categorises PTSD under seven major categories. Learning about these is crucial in understanding the differences in the subjectivity of the disorder. Trauma exposure has a large spectrum, specifically focusing on direct and indirect trauma. A “witnessed” trauma is the most commonly experienced compared to a direct trauma, where an individual psychologically or physiologically endures the experience firsthand. Following trauma, PTSD occurs as a relapse to the traumatic instance. This may present as PTSD or CPTD. It is very crucial to raise awareness of the difference between the two terms for effective diagnosis and countermeasures, as CPTSD is also commonly associated with BPD. The levels of neuroplasticity occurring in the hippocampus solely depend on the external environment of an individual. Effectors such as ACEs during childhood present dire consequences for the development of the immature brain. These consequences impact the capacity growth of episodic memory for a growing child.
This elaborate review reflects the subjective nature of trauma. The research demonstrates how each individual has their own way of interpreting an experience and how ACEs can shape an individual’s life in the long-term. In closing, we firmly believe that diagnosing each case independently without bias is the ideal way to move forward with studies on this topic and that preventing or mitigating these experiences through improved policies and education is of the utmost importance.
Bibliography
Aces Aware (2021). Adverse Childhood Experiences and Related Life Events. Aces Aware [online]. <https://www.acesaware.org/wp-content/uploads/2021/07/ACEs-Aware-Practice-Paper-WYS-and-MRC-6.28.21.pdf>
American Psychiatric Association (2022). Diagnostic and statistical manual of mental disorders (DSM-5-TR). American Psychiatric Association [online]. <https://www.psychiatry.org/psychiatrists/practice/dsm>
American Psychological Association (2018). “Self-enhancement”. APA Dictionary of Psychology [online]. <https://dictionary.apa.org/self-enhancement>
American Psychological Association (2025). American Psychological Association [online]. <https://www.apa.org/>
Assink, M., Spruit, A., Schuts, M., Lindauer, R., van der Put, C.E. & Stams, G.-J.J.M. (2018a). The intergenerational transmission of child maltreatment: A three-level meta-analysis. Child Abuse & Neglect, 84(84), pp.131–145.
Assink, M., Spruit, A., Schuts, M., Lindauer, R., van der Put, C.E. & Stams, G.-J.J.M. (2018b). The intergenerational transmission of child maltreatment: A three-level meta-analysis. Child Abuse & Neglect, 84(84), pp.131–145.
Baumrind, D. (1966). Effects of Authoritative Parental Control on Child Behavior. Child Development, 37(4), pp.887–907.
Blum, K. (2024). The Impact of Chronic Stress on Brain Function and Structure. Neuroscience and Psychiatry: Open Access, 7(5), pp.262–264.
Bremner, J.D. (2006). Traumatic stress: effects on the brain. Dialogues in Clinical Neuroscience, 8(4), pp.445–461.
Brody, G.H. & Flor, D.L. (1998). Maternal Resources, Parenting Practices, and Child Competence in Rural, Single-Parent African American Families. Child Development, 69(3), p.803.
Catalyst Care Group (2025). Adverse Childhood Experiences: Impact and Insights. Catalyst Care Group [online]. <https://catalystgrp.co.uk/blog/adverse-childhood-experiences-impact-and-insights/>
CDC (2024). A Public Health Approach to Adverse Childhood Experiences. CDC [online]. <https://www.cdc.gov/aces/php/public-health-strategy/index.html>
Chao, R.K. (1994). Beyond Parental Control and Authoritarian Parenting Style: Understanding Chinese Parenting through the Cultural Notion of Training. Child Development, 65(4), pp.1111-1119.
Cisler, J.M. & Herringa, R.J. (2021). Posttraumatic Stress Disorder and the Developing Adolescent Brain. Biological Psychiatry, 89(2), pp.144–151.
Cumberland Council (2022). Chapter 3: Understanding trauma and adversity’s impact on mental health. Cumberland Public Health Annual Report, 2023/4 [online]. <https://www.cumberland.gov.uk/cumberland-public-health-annual-report-20234/chapter-3-understanding-trauma-and-adversitys-impact-mental-health>
Dariotis, J.K., Chen, F.R., Park, Y.R., Nowak, M.K., French, K.M. & Codamon, A.M. (2023). Parentification vulnerability, reactivity, resilience, and thriving: A mixed methods systematic literature review. International Journal of Environmental Research and Public Health, 20(13), pp.6197–6197.
Dickson, D.J., Laursen, B., Valdes, O. & Stattin, H. (2019). Derisive Parenting Fosters Dysregulated Anger in Adolescent Children and Subsequent Difficulties with Peers. Journal of Youth and Adolescence, 48(8), pp.1567–1579.
Donagh, B., Taylor, J., al Mushaikhi, M. & Bradbury-Jones, C. (2022). Sibling Experiences of Adverse Childhood Experiences: A Scoping Review. Trauma, Violence, & Abuse, 24(5), p.152483802211342.
Ellis, W.R. & Dietz, W.H. (2017). A New Framework for Addressing Adverse Childhood and Community Experiences: The Building Community Resilience Model. Academic Pediatrics, 17(7S), pp.S86–S93.
Esposito, C., Miranda, M.C., Rothenberg, W.A., Skinner, A.T., Lansford, J.E. et al. (2025). Parent–adolescent discrepancies in perceptions of parental warmth: Cross‐cultural differences and longitudinal associations with internalizing symptoms. Journal of Research on Adolescence, 35(4), pp.e70093–e70093.
Evans‐Strong, A., Walton, N., Blandino, K., Roper, A.T.C., Donaldson, S.T., Lewis, M. & Maguire, J. (2024). Witnessed trauma exposure induces fear in mice through a reduction in endogenous neurosteroid synthesis. Journal of Neuroendocrinology, 36(4).
Feriante, J. & Sharma, N.P. (2023). Acute and Chronic Mental Health Trauma. National Library of Medicine [online]. <https://www.ncbi.nlm.nih.gov/books/NBK594231/>
First Things First (2018). Brain Development. First Things First [online]. <https://www.firstthingsfirst.org/early-childhood-matters/brain-development/>
Friedman, M. (2025). History of PTSD in veterans: Civil war to DSM-5. U.S. Department of Veterans Affairs [online]. <https://www.ptsd.va.gov/understand/what/history_ptsd.asp>
Giotakos, O. (2020). Neurobiology of emotional trauma. Psychiatriki, 31(2), pp.162–171.
Greiner, S.-K., Pons, M.D., Ablimit, A., Brauße, E., Adorjan, K., et al. (2025). How childhood adversities shape minds and lives: An analysis across the affective-to-psychotic spectrum. Psychiatry Research, 350, p.116536.
Guy-Evans, O. (2021). Fight, Flight, Freeze, or Fawn: How We Respond to Threats. Simply Psychology [online]. <https://www.simplypsychology.org/fight-flight-freeze-fawn.html>
Han, H., Koziol-McLain, J., Diesfeld, K., Carrington, S.D., Morse, Z. & Lees, A.B. (2024). Protecting children in Aotearoa New Zealand: a review on legal and professional frameworks for oral health practitioners. Journal of the Royal Society of New Zealand, 55, pp.1–14.
Hofstede, G. (2001). Culture’s consequences: Comparing values, behaviors, institutions, and Organizations across Nations. Behaviour Research and Therapy, 41(7), pp.861–862.
Kagitcibasi, C. (2017). Family, Self, and Human Development Across Cultures. (Routledge).
Kaiser, A.P., Davison, E., Moye, J., Spiro, A. & Larsen, S.(2014). PTSD Assessment and Treatment in Older Adults. U.S. Department of Veterans Affairs [online]. <https://www.ptsd.va.gov/professional/treat/specific/assess_tx_older_adults.asp>
Katembu, S., Zahedi, A. and Sommer, W. (2023). Childhood Trauma and Violent Behavior in Adolescents Are Differentially Related to cognitive-emotional Deficits. Frontiers in Public Health, 11(1001132).
Kearney, B.E. & Lanius, R.A. (2022). The brain-body disconnect: A somatic sensory basis for trauma-related disorders. Frontiers in Neuroscience, 16(16).
Kuppens, S. & Ceulemans, E. (2019). Parenting styles: A closer look at a well-known concept. Journal of Child and Family Studies, 28(1), pp.168–181.
Læknablaðið. (2023). Tengsl langvinnra verkja á fullorðinsárum og sálrænna áfalla í æsku. Læknablaðið [online]. <https://www.laeknabladid.is/tolublod/2023/02/nr/8223>
Lau, E.Y.H. & Power, T.G. (2019). Coparenting, Parenting Stress, and Authoritative Parenting among Hong Kong Chinese Mothers and Fathers. Parenting, 20(3), pp.1–10.
Lee, J.K., Johnson, E.G. & Ghetti, S. (2017). Hippocampal Development: Structure, Function and Implications. The Hippocampus from Cells to Systems, pp.141–166.
Little, M.A. (2024). How Permissive Parents Hurt Their Children. Psychology Today [online]. <https://www.psychologytoday.com/us/blog/childhood-narcissism/202410/how-permissive-parents-hurt-their-children?msockid=1fc32d9086f967283f9f3e9c874b66d4>
Lu, S., Xu, Y., Cui, D., Hu, S., Huang, M., Li, L. & Zhang, L. (2024). Exploring the association between childhood trauma and limbic system subregion volumes in healthy individuals: a neuroimaging study. BMC Psychiatry, 24(1).
McCormack, D., Subburamu, S., Guzman, G., Calderon, C., Darapaneni, R., Lis, R., Sima, N., Sperling, J. & Corbo, J. (2022). Traumatic Injuries in Sexual Assault Patients in the Emergency Department. Western Journal of Emergency Medicine, 23(5), pp.672–677.
Mind (2023). Effects of trauma. Mind [online]. <https://www.mind.org.uk/information-support/types-of-mental-health-problems/trauma/effects-of-trauma/>
Muhammad, N., Sayema, R., Rathi, B., Baroi, J. & Islam, J. (2021). Parenting Style and Aggressive Behavior Among High School Children. Parenting Style and Aggressive Behavior Among High School Children, 6(2), pp.123–134.
Mureșanu, I.A., Grad, D.A., Mureșanu, D.F., Dobran, S.-A., Hapca, E., Strilciuc, Ș., Benedek, I., Capriș, D., Popescu, B.O., Perju-Dumbravă, L. & Cherecheș, R.M. (2022). Evaluation of post-traumatic stress disorder (PTSD) and related comorbidities in clinical studies. Journal of Medicine and Life, 15(4), pp.436–442.
Murphy, D., Karatzias, T., Busuttil, W., Greenberg, N. & Shevlin, M. (2021). ICD-11 posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) in treatment seeking veterans: risk factors and comorbidity. Social Psychiatry and Psychiatric Epidemiology, 56(8).
National Institute of Mental Health (2023). Post-Traumatic Stress Disorder. National Institute of Mental Health [online]. <https://www.nimh.nih.gov/health/publications/post-traumatic-stress-disorder-ptsd>
NHS (2022). Post-traumatic Stress Disorder. National Health Service [online]. <https://www.nhs.uk/mental-health/conditions/post-traumatic-stress-disorder-ptsd/overview/>
Palumbo, A. (2023). Narcissistic Parenting and its Effects on Parenting Styles and Narcissistic Parenting and its Effects on Parenting Styles and Child Development Child Development. Virtual Commons Bridgewater State University[online]. <https://vc.bridgew.edu/cgi/viewcontent.cgi?article=1628&context=honors_proj>
Pardee, M., Kuzma, E., Dahlem, C.H. (Gina) Y., Boucher, N. & Darling-Fisher, C.S. (2017). Current state of screening high-ACE youth and emerging adults in primary care. Journal of the American Association of Nurse Practitioners, 29(12), pp.716–724.
PhD in Parenting (2016). Parenting styles to the extreme. PhD in Parenting [online]. <https://www.phdinparenting.com/blog/2010/12/2/parenting-styles-to-the-extreme.html>
Prevoo, M.J. & Tamis-LeMonda, C.S. (2017). Parenting and globalization in western countries: explaining differences in parent–child interactions. Current Opinion in Psychology, 15, pp.33–39.
Psychology Today (2023). Parentification. Psychology Today [online]. <https://www.psychologytoday.com/us/basics/parentification#healing-from-parentification>
Psychology Today (2024). Maybe You’re Not an Introvert. Maybe It’s a Trauma Response. Psychology Today [online]. <https://www.psychologytoday.com/us/blog/targeted-parenting/202412/maybe-youre-not-an-introvert-maybe-its-a-trauma-response>
SAMHSA (2014). Understanding the Impact of Trauma. Trauma-Informed Care in Behavioral Health Services.
Schroeder, K., Schuler, B.R., Kobulsky, J.M. & Sarwer, D.B. (2021). The association between adverse childhood experiences and childhood obesity: A systematic review. Obesity Reviews, 22(7).
Scott, R. & Freckelton, I. (2024). Vicarious trauma among legal practitioners and judicial officers. Psychiatry Psychology and Law, 31(3), pp.500–522.
Silva, C., Moreira, P., Moreira, D.S., Rafael, F., Rodrigues, A., Leite, Â., Lopes, S. & Moreira, D. (2024). Impact of Adverse Childhood Experiences in Young Adults and Adults: A Systematic Literature Review. Pediatric Reports, 16(2), pp.461–481.
Tamir, T.T., Tekeba, B., Mekonen, E.G., Gebrehana, D.A. & Zegeye, A.F. (2025). Shadows of trauma: an umbrella review of the prevalence and risk factors of post-traumatic stress disorder in children and adolescents. Child and Adolescent Psychiatry and Mental Health, 19(1).
The National Child Traumatic Stress Network (2023). About Child Trauma. The National Child Traumatic Stress Network [online]. <https://www.nctsn.org/what-is-child-trauma/about-child-trauma>
Van der Kolk, B. (2000). Posttraumatic stress disorder and the nature of trauma. Posttraumatic Stress Disorder, 2(1), pp.7–22.
Vigdal, J.S. & Brønnick, K.K. (2022). A Systematic Review of ‘Helicopter Parenting’ and Its Relationship With Anxiety and Depression. Frontiers in Psychology, 13(13).
World Health Organization (2024). Post-traumatic Stress Disorder. World Health Organization [online]. <https://www.who.int/news-room/fact-sheets/detail/post-traumatic-stress-disorder>
Zarse, E.M., Neff, M.R., Yoder, R., Hulvershorn, L., Chambers, J.E. & Chambers, R.A. (2019a). The adverse childhood experiences questionnaire: two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Medicine, 6(1).
Zarse, E.M., Neff, M.R., Yoder, R., Hulvershorn, L., Chambers, J.E. and Chambers, R.A. (2019b). The adverse childhood experiences questionnaire: two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Medicine, 6(1).




{kind=link}